Download
1 / 52
530 likes | 727 Views
Hernias, Heartburn, and Balloons. Ahmed R Ahmed Consultant in Laparoscopic, Upper GI and Bariatric Surgery Clinical Lead – Bariatric Services Imperial College London Director of Surgery Bupa Cromwell Hospital Weight Management Centre.

E N D
Hernias, Heartburn, and Balloons Ahmed R Ahmed Consultant in Laparoscopic, Upper GI and Bariatric Surgery Clinical Lead – Bariatric Services Imperial College London Director of Surgery Bupa Cromwell Hospital Weight Management Centre
“You can judge the worth of a surgeon by the way he does a hernia” Sir Thomas Fairbank
“There is no doubt that the first appearance of the mammal, with his unexplained need to push his testicles out of their proper home into the air, made a mess of the three layered abdominal wall that had done the reptiles well for 200 million years” William Ogilvie
A common, established procedure • Open repair is the preferred operation for primary inguinal herniorrhaphy by 86% of surgeons in the US. Rutkow IM. Demographic and socioeconomic aspects of hernia repair in the United States in 2003. Surg Clin N Am 2003; 83:1045–51.
Open herniorraphy • Short learning curve • Cheap • Less chance of recurrence • Can be done under local anaesthetic
Laparoscopic repair • is the technique safe? • is the repair secure? • are long-term morbidity rates better than in open repair? • do patients return to normal activities and work earlier? • and are there any additional benefits?
Is the technique safe? • The EU Hernia Trialists Collaboration • Meta-analysis of 34 eligible trials (RCTs) with a total of 6804 patients. • Complications reduce with experience • Laparoscopic complications show a marked improvement between the early and late 1990s with an incidence of 5.6% and 0.5%, respectively (P < 0.001). • Haematoma occurs more frequently after open surgery. • Testicular injury and wound infection is more common after open repair EU Hernia Trialists Collaborative. Br J Surg 2000; 87: 860–7.
Is the repair secure? 34 TRIALS ANALYSED RECURRENCES *10 RCTs comparing TAPP with open repair and 4 RCTs comparing TEP with open repair Prof Grant. EU Hernia Trialists Collaborative. Br J Surg 2000; 87: 860–7.
Are postop morbidity rates better? • 5-year follow-up of 400 patients treated with either Lichtenstein open mesh repair or TAPP repair • the incidence of permanent paraesthesia: 23% vs 3% • groin pain 10% vs 2% • all of the patients with pain and paraesthesia significant enough to affect their daily lives were in the open repair group Wellwood: Prospective randomized controlled trial of laparoscopic versus open inguinal hernia mesh repair: five year follow up. BMJ 326:1012, 2003
Do patients return to normal activitiesand work earlier? • 27 RCTs have considered the speed of recovery and return to work. • 24 of these report an earlier return to both activity and work in the laparoscopic groups compared with open repair. • This is estimated to equate to an absolute difference of about 7 days in terms of time off work. McCormack K, Scott NW, Go PM, Ross S, Grant AM and EU Hernia Trialists Collaboration. Laparoscopic techniques versus open techniques for inguinal hernia repair. Cochrane Databases System Rev 2003(1); CD 001785.
Are there any additional benefits? • Laparoscopic surgery allows bilateral hernias to be repaired through the same three small incisions • there is no increase in postoperative pain or recovery time • The same advantages are apparent in the repair of recurrent hernias particularly when the recurrence has occurred more than once
Is laparoscopic repair cost effective? • Both laparoscopic and open techniques can be routinely performed as day cases in fit patients • Societal costs due to quicker recovery and return to employment show clear advantages for the laparoscopic repair. Hospital Episode Statistics 2001/2 http:/www.doh.gov.uk/hes/freedata/index.html
Hiatus (Paraesophageal) hernias Type 1 paraesophageal hernia
Paraesophageal hernias Type 2 hernia Type 3 hernia
Clinical features • Asymptomatic • Major • Minor • Emergency
Clinical features • Asymptomatic • Stomach freely herniates and reduces through a open hiatus
Clinical features • Major symptoms • Postprandial chest pain (74%) • Dysphagia (60%) • Anemia (30%) • Strangulation > ischaemia > bleeding • Venous engorgement > chronic oozing • Cameron’s ulcer • Pulmonary problems (44%) • Loss of intrathoracic volume • aspiration
Clinical features • Minor symptoms • Regurgitation (77%) • Heartburn (60%) • Nausea and/or vomiting (35%)
Clinical features • Emergency = volvulus • Severe pain • Bleeding • Perforation > Peritonitis and sepsis* * 50% mortality rate > case for elective repair strangulation
Diagnostic Methods • Upper gastrointestinal contrast study • CT • Gastroscopy
Controversies • Do all paraesophageal hernias require repair?
Principles of surgical repair Standard principles of hernia repair apply: • free the sac • reduce the hernia • repair the defect
How to close the crural defect? Primary suture cruroplasty
How to close the crural defect? Cruroplasty reinforced by mesh
Weight loss - Treatment options Lifestyle Modifications e.g. diet and exercise Anti-obesity medications - Xenical® (Orlistat/Alli) Surgery (in suitable patients – NOCE, NIH criteria)
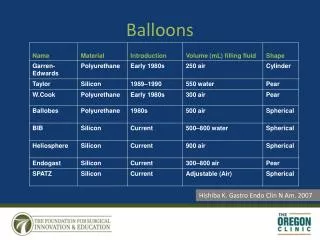
Weight loss Healthy Weight (BMI 18.5 to 24.9) Overweight(BMI 25 to 29.9) Obese(BMI 30 to 34.9) Severely Obese(BMI 35 to 39.9 ) Morbidly Obese(BMI 40 or more) BARIATRIC SURGERY GASTRIC BALLOON
The Intragastric Balloon An option between diets and surgical treatment
Treating obesity with an Intragastric Balloon The balloon itself The Intragastric Balloon is a weight-loss system Education about weight-loss
Who is suitable? Motivated, moderately obese adults. BMI of 27 and over Prepared to make changes in eating habits and lifestyleWilling to work with medical team and attend meetings.
The procedure Step 1 Assessment Step 2 Insertion Step 3Follow upDiet and changed eating habitsExercise Step 4 Removal Maintain weight-loss
Balloon removal Removal of the balloon follows the same simple procedure as placementA tube is passed into the stomach and the balloon is deflatedThe deflated balloon is then removed through the mouthPatients can usually return home within hours
Following the procedure • Regular scheduled meetings with the team to continue education and support on new eating and exercise habits • The balloon helps adjustment to reduced caloric intake by producing a feeling of satiety • 15-20 Kgs weight loss / 6 months
Life after balloon removal Balloon removal after six monthsKeep practicing the principlesKeep meeting with the teamNutrition, balance, exerciseMotivation remains the key to success
Benefits of theintragastric balloon programme No surgery is required No long-term use of pharmaceuticals Feeling of satiety makes success more likely than other programmes 10-20Kgs / 6 months
Intragastric balloon Possible indications • Hard to control co-morbidities in lower BMI >Diabetes / Hypertension weight = control
Intragastric balloon Possible indications • Weight loss to improve surgical condition in non bariatric operations > Orthopaedic surgery • Joints • Spine
Intragastric balloon Possible indications • Infertility • Effective weight loss > Improves women fertility
Intragastric balloon Possible indications • Weight loss post “pregnancy obesity” > Woman should loose all the weight gain in pregnancy with breast feeding • But... • It is not what we see in consecutive pregnancies
Intragastric balloon Possible indications • Aesthetics >“Preparing for special happenings” >“Psychological well being” >“ less risky than liposuction”