Download
1 / 58
1.15k likes | 3.87k Views
DERM: Topical steroids scabies Acne alopecia Rosacea Antifungals Immunomodulators. Topical Corticosteroids . Nursing 7755 Fall 2010 Debkfp@hotmail.com. Topical corticosteroids. MOA: Vasoconstriction Anti-inflammation Decrease epidermal proliferation. Cell. Inhibit phospholipase

E N D
DERM: Topical steroids scabies Acne alopecia Rosacea Antifungals Immunomodulators Topical Corticosteroids Nursing 7755 Fall 2010 Debkfp@hotmail.com
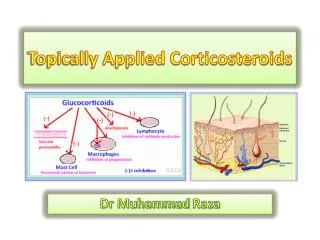
Topical corticosteroids MOA: Vasoconstriction Anti-inflammation Decrease epidermal proliferation Cell Inhibit phospholipase A2 which reduces skin levels of pro-inflam kinines: Arachidonic acid (Omega-6, ’s inflammation) Prostaglandins (’s vascular dilation) Leukotrienes (inflammatory response)
USE: erythema, scaling & pruritus lichen planus lichen sclerosis atopic dermatitis lichen simplex chronicus nummular eczema psoriasis asteatotic dermatitis
Uses, cont. Severe ezcema alopecia areata discoid lupus severe poison ivy
SE’s • Systemic: • Suppression of HPA axis • Hyperglycemia Cushinoid features Steroid induced Acne
SE Long-term use : • Local tissue atrophy w/ striae • Thinning of epidermis w/ telangiectasias & purpura • Masking bacterial or fungal infx • Skin fragility
Choosing a topical steroid • many topical steroids available • different vehicles • differ in potency and formulation • Weaker: thin-skinned, sensitive areas • axillae, groin, perianal, breast folds, face, eyelids • Moderate: • trunk, arms, legs • Strong: thick-skinned areas • palms, soles, certain dermatitis such as lichen planus and psoriasis
Altering Corticosteroids In 1952 basic cyclopentanophenanthrene nucleus .. three 6-carbon rings (A, B, C) + a single 5-carbon ring (D numerous modifications: • alterations affect potency, pharmacodynamic activity, adverse reaction risk • potency is significantly increased by modifications at: • C-6a or C-9a Fluorination • C-21 Halogenation • C-17. C-21 Esterification • Double bond between C-1 and C-2 on ring A.
Ointments • Most effective • Ointment have oily/greasy base (ie:petroleum jelly) • Greasy texture persists on the skin surface • Translucent • Best lubrication, penetration • Best for dry or thick, hyperkeratotic lesions • Not recommended for areas where skin touches skin or acutevesicular or weeping rashes • poor pt satisfaction / compliance b/c grease
Creams • most often prescribed • water suspended in oil • white color/ less greasy/ vanish into the skin • good lubricating/ emollient qualities • USE: • most skin areas, useful where skin touches skin (groin, rectal area, armpits ) • acute exudative inflammation b/c of drying effect w/ repeated use • generally less potent than ointments of the same medication, • often contain preservatives (cause irritation, stinging, allergic reaction)
Lotions and gels • Solution or lotion: bases contain water, alcohol, • other chemicals • Clear or milky appearance • least greasy & occlusive • drying effect on an oozing lesion • useful for use on the scalp b/c no residue • can cause stinging and drying Foams: Use: hairy areas expensive drying • Gels: mixture of propylene glycol (drying) & water • Clear color, nongreasy, • jelly-like consistency • Use: exudative inflammation(poison ivy) • "wet" rashes ,scalp Cordran tape
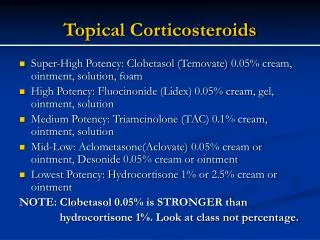
Potency • There are seven groups of topical steroid potency, ranging from ultra high potency (group I) to low potency (group VII). • Fluorinated topical steroids are generally more potent than others • IE: triamcinolone acetonide (contains fluoride ion) is 100x more potent than nonfluorinated HC
II: High Betamethasone dipropionate 0.05% AF cream, lotion (DiproleneAF) Fluocinonide 0.05% gel, cream, oint, sol (derma-smoothe, Lidex) Mometasone fuorate 0.1% lotion oint (Elecon) Potency: 7 groups-- I: High-> VII:low I :Ultra High Betamethasone dipropionate 0.05%Gel, oint (Diprolene) Clobetasol propionate 0.05%cr, oint, sol, foam(Temovate, Olux) Halobetasol propionate 0.05%cr, oint. (Ultravate)
Potency III: Medium to high Betamethasone dipropionate 0.05% cream Betamethasone valerate 0.05% 0.1% lotion oint Fluticasone propionate 0.05% oint Triamcinolone acetonide 0.1% oint, 0.5%cream IV: Medium Betamethasone benzoate 0.025% oint Betamethasone valerate 0.12% Luxiq foam Fluocinolone acetonide 0.025% oint Fluticasone propionate 0.05% cream Hydrocortisone valerate 0.2% oint Triamcinolone acetonide 0.1 cream
Potency V:Medium Low Betamethasone dipropionate 0.05% lotion Betamethasone valerate 0.01%0.05% 0.1% cream Fluticasone acetonide 0.025% cream Hydrocortisone valerate 0.2% cream Triamcinolone acetonide 0.1% lotion VI :Low Fluticasone acetonide 0.01% cream/ solution Triamcinolone acetonide 0.1% cream (Aristocort) VII: Least potent Hydrocortisone 1%, 2.5% cr, lotion, oint Dexamethasone 0.1% gel, aerosol,cream Methylprednisolone acetate0.25%, 1% cream oint
Combo product • Lotrisone, Mycolog II: potent steroid plus antifungal
Application tips • Children/elderly: • avoid potent fluorinated compounds • Face: • only non-fluorinated • mild unless severe dematitis • Better to use super-potent briefly than mild • ineffective long term
Frequency of Administration • QD or BID application • No improved result for more frequent administration • Chronic application can induce tachyphylaxis (tolerance) • Max 3wks for ultra-high-potency steroids
Amount of application • Titrate to the minimal amt needed • Prevent tachyphylaxis: • 1wk on, 1wk off or 3d on,4d off • taper off • hi potent for flare, low for control. • Amount: does not affect penetration or potency • Thick application is wasted • Only thin layer in intimate contact w/ skin is absorbed • Absorption: Thin to thick stratum corneum: mucous membranes -> scrotum-> eyelids-> face-> torso-> extremities-> palm,soles, elbows, knees • Inflamed skin: less barrier, better absorption
Dosing-FTU 2 FTU = 1gm
Occlusion • Occlusion: determines penetration • Occlusion: ’s hydration-> ’s penetration-> ’s potency • Intertriginous: touching skin acts like occlusive dssg (axillae, inguinal) • Create Occlusion: non-breathing saran wrap, held by tape, sock, Ace; leave on all noc • ie plastic shower cap; cordran tape rubber gloves, baggies, sauna suits.
Application tips • Stratum corneum acts as reservoir • continues to release med. • So apply qd • Decreasing epidermal barrier: • Soaking to hydrate stratum corneum--> better penetration; • Wrinkling ’s skins surface area to accomodate water it absorbs • Smearing: after soaking, smear onto wet skin to trap absorbed water
Sulfacetamide • -Klaron • -Plexion • -Rosac • -Rosanil • -Rosula • -Sulfacet R Acne meds topical • Clindamycin Top • CleocinT • Clindagel • Clindamax • Evoclin • Clindamycin/BPO • Acanya • BenzaClin • Duac • Clindamycin/tretinoin • Ziana • Erythromycin top • Akne-mycin • Erythro/BPO • Benzamycin Azelaic acid • Azelex • Finacea Dapsone • Aczone Benzoyl peroxide • Benzac AC • Benzac W • Brevoxyl • Desquam E • Desquam X • Triaz • ZoDerm • RETINOIDS: • Adapalene • Differin • Adapalene/BPO • Epiduo • Tazarotene • -Tazorac • Tretinoin Topical • Atralin • Avita • -RetinA • -RetinA micro
BENZOYL PEROXIDE • Works as peeling agent • ’s cell sloughing/ skin turnover • Loosens follicular plug • Works as direct antimicrobial against p.acnes.. • BPO is decomposed on skin by cysteine-> • Liberating free Oxygen radicals-> • That oxidize bacterial proteins • Applysparingly,to dry skin, 30”after washing, the lowest concentration, taper up,qod->tid Acne… papular • Forms:Soap, lotion, cream, wash, gel:more stability, more potent; alcohol or water based, alcohol base more drying, irritating • 1-10% • 5 &10% not signif. more effective than 2.5% • 2.5% is better tolerated • Add 10%urea:moisturizing Preg: C SE: initial dryness, irritation; develops tolerance 1+wk; Misc:Reduces anbx resistance if used w/anbx; bleach fabrics
Clindamycin:anti-inflam, comedolytic • Gel, lotion, sol, foam, pads • BID; better w/ BPO • SE: rash, GI/diarrhea • Preg B Topical Anbx pustular cystic • Erythromycin: • blocks cell wall synthesis • 1%-4% w/ w/o zinc (enhances penetration) • Gel, lotion, solution , pads • SE: erythema, dryness • Apply bid, Preg B • W/ BPO more effective Sulfacetamide:sulfa anbx inhibits folate synthesis SE: local irritation, burning, itching erythema, SJS Avoid w/sulfa allergy Apply thin film BID Preg C
Topical Acne cont.antibacterial / anti-inflammatory Azelaic acid: found in wheat, rye, barley. Naturally produced by Malassezia furfur (AKA Pityrosporum ovale), a normal skin yeast. MOA: unknown Antibacterial: (Propionibacterium acnes & Staphylococcus epi) Keratolytic / comedolytic: Normalizes lining of hair follicle. Antiinflammatory Reduces pigmentation: melasma, actinic lentigines. USE: >12yr, clean/dry skin BID SE: skin irritant, hypopigmentation Preg: B Dapsone (leprosy) antibacterial, anti-inflammatory Adv. Rx: Facial edema, depression, psychosis, tonic clonic sz, sinusitis, Abd pain, pancreatitis, vomiting Apply: pea-sized amt, thin layer BID; reevaluate if no improvement after 12wk SE: Yellow/orange color of skin & hair w/ dapsone gel + top.BPO DI: trimethoprim Preg: C Monitor: CBC
Uses: • 1st w/ mild/mod infammatory or pustular acne, • fine wrinkles • hyperpigmentation • tactile roughness Topical…..Retinoids *Use with BPO or top anbx MOA: Vitamin A derivative • Anti-inflammatory • Exfoliating • Comedolytic:’s cell turnover in follicular wall, ’s cohesiveness of cells ’s stratum corneum cell layers from 14 to 5 Apply: • qhs/qohs, 30”after washing • Initial flare / results 8-12wk • Apply 3-5”prior to top clinda Enhances penetration (&SE) of topical clinda. • Synergistic w/ BPO; use BPO qam/tretinoin HS, enhance efficacy w/ less irritation SE: *Irritation Stinging *Dryness Pruritus *Erythema Burning *Photosensitivity Hypertriglyceridemia ?? AGE: Not <12yr Preg: C (po teratogenic) DI:Substrate of minor:CYP2A6, 2B6, major 2C8,2C9 Inhibits weak CYP2C9 Induces weak CYP2E1 OCPs (’s progestin concentration)
RETINOIDS: • Tretinoin Topical • Atralin • Avita • -RetinA • -RetinA micro • Adapalene • Differin • Adapalene/BPO • Epiduo • Tazarotene • -Tazorac Retinoids… Tretinoin:… Solution: (most irritation) 0.05% solution Gels: 0.01% and 0.025% gels Gel microsphere: 0.04%, 0.1% Creams: (least irritation) 0.025% cream (mild, sensitive skin) 0.05% cream (mod, sensitive skin) 0.1% creams (mod, nonsensitive skin) • Adapalene: 3rd gen retinoid: 0.1% gel, crm, alcoholic sol, pledgets, 0.3% gel • 0.1% gel better tolerable than tretinoin 0.025% gel • More selective binding for retinoid acid receptor in epidermis • Tazarotene: prodrug, synthetic retinoid, converted to active form of tazarotenic acid after application; selective binding to RARs • 0.1%, 0.05% gel & crm • more effective than 0.025% tretinoin gel, 0.1%, microsphere, adapalene 0.1% gel • SE: peri-lesional irritation
Acne meds oral www.ipledgeprogram.com Black Box: teratogenicity (2 forms of birth control) SE: depression/ suicide etc CBC changes Rashes (SJS) Pseudotumor cerebri Common Rx: Chelitis, dry skin, pruritus Conjunctivitis, photosensitivity Hypertrigs Hair loss Visual disturbances Monitoring: Check LFTs, trigs, Hcg qmo • Isotretinoin $$$ • Accutane tier 3/na • Amnesteem t 1 • Claravis t 1 • Sotret t 1 • doxycycline 100mg qd..$free • Adoxa t3 • Doryx t3 • Monodox t3 • Oracea t3 • minocycline t1 50mg 1-3x/d $15/30 • Solodyn t3 SE: Yeast Caution<8yr Tooth discolor Photosensitivity GI upset Separate from dairy Avoid <8yr; Preg D Monitor CBC, LFT, BUN/CR
Rosacea • acneiform disorder of middle-aged & older adults • characterized by vascular dilation of central face • (nose, cheek, eyelids, forehead.) The disease is chronic; control rather than cure is the goal of therapy.
ROSACEA Topical antibiotics & BPO relieve inflammation • Sodium sulfacetamide 10%/sulfur 5 % lotion • Clindamycin 1% solution, gel, lotion • Erythromycin 2% solution BID, somewhat less effective than other anbx • Benzoyl peroxide 2.5% QD/BID, increasing to 5 or 10 %, Effect: 4-6wk • For papular and pustular lesions : • thin layer, entire involved area, QD/BID • Metronidazole: w/ or w/o short course of oral antibiotics. • QD:1% gel (30g) qd • BID: 0.75% cream (45g), lotion (59mL), 0.75% gel (28.4g) • “Metrocream” “MetroLotion” “Metrogel” • Azelaic acid: sl more effective/more irritating • 20% cream (30 g) BID; 15% gel BID “Azelex”, “Finacea” Combination products (eg, benzoyl peroxide + erythromycin “Benzamycin” benzoyl peroxide + clindamycin) “Benzaclin” ”Duac”
Topical Antifungals IMADAZOLES POLYENE • miconazole • Zeasorb AF • Micatin otc • Neosporin AF OTC • Monistat derm • Fungoid tincture0tc • Lotrimin AF Spray OTC • miconazole/petrolatum/ zn oxide • Vusion • ketoconazole • Extina • Nizoral AD OTC • Nizoral • Xolegel • oxiconazole • Oxistat • clotrimazole • Mycelex • nystatin/triamcinolone • Mycolog II • nystatin topical • Mycostatin • Nyanyc • Pedi Dri OTHER butenafine Mentax Lotrimin ultra otc terbinafine Lamisil AT otc naftifine Naftin • selenium sulfide OTC • Selsun • Selsun blue OTC • phenol: • OTC: castellani Paint modified ALLYLAMINES • tolnaftate • LamisilAF otc • Tinactin • ciclopirox • Penlac Nail Lacquer • Loprox • Gentian violet otc clotrimazole/betameth. Lotrisone Econazole Spectazole
Oral antifungals Imidazole, triazole, thiazole antifungals Echinocandin anidulafungin Eraxis caspofungin Cancidas micafungin Mycamine • Imidazole: • ketoconazole • clotrimazole • Mycelex Polyene antifungals Amphotericin B Abelcet AmBisome Amphocin Amphotec Nystatin • Triazoles: • fluconazole • Difucan • itraconazole • Sporonox • voriconazole • Vfend • posaconazole • Noxafil other griseofulvin: Grifulvin V. Gris-PEG flucytosine Ancobon (Antimetabolite) Allylamines terbinafine Lamisil
antifungals USE: fungalinfections ie: candidiasis tinea pedis tinea corporis KOH..hyphae
Polyene antifungals • bind with ergosterol in the fungal cell membrane, • causes the cell to leak • Animal cells contain cholesterol instead of ergosterol and so are much less susceptible. • at therapeutic doses, some amphotericin B may bind to animal membrane cholesterol, increasing the risk of human toxicity. • IV Amphotericin B is nephrotoxic.
Imidazole, triazole, and thiazole antifungals .. inhibit the enzyme lanosterol 14 α-demethylase; the enzyme necessary to convert lanosterol to ergosterol. • Different mechanism of inhibition of the CYP450 enzyme. • Imidazole: N3 of the Imidazole compound binds to CYP450, • Triazole: N4 of the Triazoles bind to CYP450 • Triazoles have higher specificity for the CYPP450 than Imidzoles, thus more potent than Imidazoles.
Allylamines …inhibit squalene epoxidase, another enzyme required for ergosterol synthesis. OTHER Griseofulvin binds to polymerizedmicrotubules and inhibits fungal mitosis DI’s: CYP3A4, increased concentration w/ CCBs, immunosuppressants, chemo drugs, benzodiazepines, tricyclic antidepressants, macrolides, SSRIs.
Topical Immuno-modulators: Protopic0.03% or 0.1% ointment& Elidel1% cream MOA: “Calcineurin” Inhibitor Inhibits T-lymphocytes & pro- inflammatory cytokines in inflamed dermis PK: Protopic substrate of CYP3A4 (major) inhibits CYP3A4 (weak), min. absorbed Elidel:substrate of CYP3A4 (minor) USE:Adult: Apply small amt 0.03% or 0.1% oint. BID rub in gently & completely. Reeval 6 wk. Child ≥2 years: use 0.03% SE: HA, burning, Black box warning ?malignancies lymphoma and skin malignancy
Aldara.. Immuno-modulator activates the body's own immune system. (cytokines, including interferon-alpha and others) no direct antiviral activity not chemodestructive or cytotoxic. USE: Perianal warts/condyloma acuminata: Apply a thin layer 3 x/wk on alternative days @hs and leave on skin for 6-10 hours. Remove by washing with mild soap and water.x<16wk. Actinic keratosis: Apply 2x/wk x 16 weeks); apply HS, leave on x8hr Common warts (unlabeled use) Apply qhs. Superficial basal cell carcinoma: Qhs 5d/wk x 6 wks. Treatment area should include a 1 cm margin of skin around the tumor. Leave on skin for 8 hours. Peds: >12yr
Lice/Scabies SCABIES:sx onset 2-6wk but contagious. Rx all household members, sexual contacts, prolonged direct skin-to-skin contact within the preceding month RX: scabicides kill mites; some kill mite eggs. • Scabicide lotion or cream: • apply to clean body, neck -> toes. • infants /young children:apply entire head / neck • leave on for the recommended time then wash • decontaminate bedding, clothing, towels used w/i 3d prior to rx, washing in hot water / drying in a hot dryer, dry-cleaning, or seal in a plastic bag x 72hrs. • Mites :survive 2-3d away from human skin. • Sx due to hypersensitivity reaction to mites & feces (scybala), • Itching may continue x several wks • If itching > 2- 4 wks after treatment-> retreat
Lice treatment • Topical pediculicides: PYRETHROIDS (permethrin, pyrethrins), malathion, lindane, benzyl alcohol. • Pyrethroids OTC Lotions (RID) 1% concentration of permethrin. • neurotoxic to lice, low mammalian toxicity, • Wash hair/towel dry hair, Saturate scalp x10”,rinse w/ water • A second treatment is indicated in 7 to 10 days, • Prescription strength permethrin (5%) available, not more effective than OTC • Malathion Rx lotion 0.5% • with terpineol was most effective at killing head lice, compared with pyrethroids and lindane • Apply x 8-12 hr. Repeat if lice noted 7-19d.
Lice rx. Benzyl alcohol 5% lotion 2009, FDA approved 6mo+ • MOA: asphyxiation of lice through obstruction of their respiratory sphericles. • Apply x 10”, saturation of scalp / hair, rinsed off with water. • Repeat in 7d • SE: irritation of skin, scalp, eyes, transient numbness at the site of application. Lindane shampoo is not a drug of first choice because it has been associated with rare neurologic adverse effects and widespread resistance. • insecticide that inhibits neurotransmission in parasitic arthropods. AE: seizures, death BLACK BOX Spinosad fermentation product of the soil bacterium Saccharopolyspora spinosa, may be a promising future treatment. MOA: compromises the CNS of lice-> paralysis. After treatment, lice free 85% spinosad, 44% permethrin.
Skin lesions… Actinic Keratoses: clone of abnormal squamous cells caused by UV light-induced gene alteration. carcinoma in situ, can develop into SCC (1:1000risk/yr) or BCC Risk : age, skin color, sun exposure. IDENTIFY: Small flat, rough papules, red, scaly patches, papules, or plaques, sun exposed areas. Seborrheic kerotosis:common epidermal tumors, benign proliferation of immature keratinocytes Age:50+,1-100s, autosomal dominant, sudden appearance of multiple seb k’sw/ skin tags & acanthosis nigricans=?malignancies;”stuck on” AKs :erythematous base, hyperkeratotic, hard or spine-like, irregular vs SebKs: smooth, sometimes soft hyperkeratosis, no erythematous base Rx:Liquid nitrogen, destructive treatment of choice topical 5-fluorouracil or imiquimod
Rx: Imiquimod, 5-FU Imiquimod/Aldara: topical immune response modifier stimulates local cytokine induction Imiquimod 5% cream; 2-3x/wk x 12-16wk complete resolution of AKs in 50% of pts, placebo 5% AE: local erythema, scabbing, flaking. Topical 5-fluorouracil: inhibits DNA synthesis, causes inflammation w/ destruction of lesion APPLY: 1-2% face, 5% elsewhere; x 2-4wk 2wk for inflammation to subside after dc’d. 4-6wk for skin to progress through erythema, blistering, necrosis w/ erosion, re-epithelialization. ALT: apply Bid until superficial ulceration occurs (2-3wk). Then:low potency topical corticosteroid cream BID to reduce inflammation until healed EFFICACY: 50% for 100 % clearance of AKs
Liquid nitrogen, LN2 • nitrogen in a liquid state at a very low temp. • cryogenic fluid which can cause rapid freezing on contact with living tissue
Skin cancers… • Squamous cell carcinoma: (SCC): common • malignant proliferation of epidermal keratinocytes • Locally invasive, usually curative. • Rarely metastasizes • Appearance: sun exposed areas; firm, flesh colored or erythematous papules or plaque • 60% start as AK • Basal cell carcinoma (BCC) common skin cancer arising from basal layer of epidermis • Low metastatic potential • Most common: southern 55-70yo cauc. female • Malignant Melanoma:aggressive, spread unpredictable, any organ • M/F White: back, extremities • Asians/Blacks: mucous membranes,soles, palms; • Risk: sun exposure, skin type, fam. hx, changing moles
Minoxidil: Rogaine (po), Mintop etc, (top) • HX: initial use: HTN • “Minoxidil may cause increased growth or darkening of fine body hairs. If this is bothersome, consult your doctor. When the medication is discontinued, the hair will return to normal within 30 to 60 days.” xxxxxxx xxxxxxxxx • 02/13/96 : patent expired • 2007 foam-based formulation of 5%
Minoxidil: MOA MOA: Unknown Vasodilator: speculated that dilating blood vessels & opening K+ channels--> allows more O2, blood & nutrients to the follicle. This causes follicles in the telogen phase to shed, usually soon to be replaced by new, thicker hairs (new anagen phase) Anagen: growth phase (2-3yrs) Catagen: regressing phase (2-3 wk) Telogen: resting phase (3mo)
Minoxidil…effectiveness, indication One study: healthy males 18-50yr w/ androgenic alopecia.. 5% sol. x 32wks: non-vellus hair counts avg 39 hairs/cm2 Placebo: 5 hairs/cm2 INDICATION: androgenic alopecia, indicated top of head only effective w/ large area effectiveness younger men (18-41yr) Alopecia areata Androgenic alopecia When DC: changes disappear w/i months
Minoxidil…SE Common: eye burning/irritation itching redness / irritation at treated area unwanted hair growth Alcohol dries scalp--> dandruff hair loss!! hairs already in telogen phase shed early, before beginning new anagen phase Severe SE: Severe allergic rx: rash hives itching SOB peripheral edema angioedema tachycardia chest tightness /pain vertigo/syncope unexplained wt gain highly toxic to cats -> death