Download
1 / 34
340 likes | 693 Views
Should Bedside Feeding Tube Placement be a New Role for Nutrition Support Dietitians? A Decision Analysis. Amy Peppard RD, LD University of Kentucky Martin School of Public Policy and Administration Masters in Health Administration Capstone Project Spring 2008. Objectives.

E N D
Should Bedside Feeding Tube Placement be a New Role for Nutrition Support Dietitians? A Decision Analysis Amy Peppard RD, LD University of Kentucky Martin School of Public Policy and Administration Masters in Health Administration Capstone Project Spring 2008
Objectives • Provide background information on feeding tubes and enteral nutrition. • Discuss the role of the nutrition support dietitian. • Review the study design and results. • Discuss recommendations based on the results of the study.
Purpose of Study • To determine if initiation of enteral nutrition is more timely if nutrition support dietitians place bedside feeding tubes instead of nurses.
Why is Nutrition Important? Crucial for the maintenance of health and prevention of disease.
Nutrition for the Critically Ill • As many as 40% of critically ill adult patients are seriously malnourished at the time of their hospital admission. • Two-thirds of all patients experience a decline in nutritional status during the length of their hospital stay. (Behara, 2008)
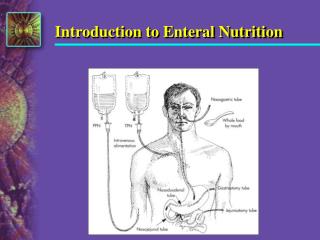
Nutrition for the Critically Ill • Patients in the intensive care unit (ICU) are often unable to consume food orally. • A feeding tube is usually placed as an alternative route to provide nutrition.
What is Enteral Nutrition? • “The provision of nutrients via the gastrointestinal tract through a feeding tube, which is the preferred route of nutrition for patients who cannot meet their nutritional needs through voluntary oral intake.” (Marian, 2007)
Research shows that early enteral nutrition in the critically ill patient decreases intestinal bacterial translocation, preserves the gut barrier and immune function, and decreases septic events. (Cresci, 2003) The Quality Management Team of the American Dietetic Association reported that initiation of enteral nutrition within the first 24 to 48 hours of injury or admission to an ICU is correlated with a decrease in infectious complications and length of hospital stay. (Kattelmann, 2008) Why is Enteral Nutrition Important?
Feeding Tube Placement • Usually the responsibility of the physician or nurse. • Other patient care responsibilities often take priority, which makes feeding tube placement difficult to perform in a timely manner. • Feeding tube placement is within the current scope of practice for nutrition support dietitians (NSDs). • Reported by the American Society of Parenteral and Enteral Nutrition (A.S.P.E.N.) Standards of Practice for NSDs. (Fuhrman, 2001)
The Role of the Dietitian • Perform nutrition assessments. • Make recommendations for nutrition support. • Monitor the patient’s tolerance of the feeding regimen. • Make any necessary changes to the nutrition care plan.
What is a Nutrition Support Dietitian? • A more specialized practice area for registered dietitians (RDs). • Board certified in nutrition support. • Deals mainly with providing patients alternative forms of nutrition in the ICU setting. • Often a member of a nutrition support team.
Organizational Setting • University of Kentucky (UK) Hospital. • 489 bed academic medical center. • Only Level I trauma center in the region. • Seven ICUs (54 beds). • Established nutrition support team.
Data Source • Data from any adult ICU patient requiring enteral nutrition. • Inclusion Criteria: • Adult patients with a feeding tube that was placed at the bedside by nursing. • Not excluded based on age, gender, or diagnosis. • Exclusion Criteria: • Patients with a surgically, fluoroscopically, or endoscopically placed tube. • Children.
Data Collection • 25 patients studied during February and March 2008. • UK Hospital’s order entry system, Sunrise Clinical Manager (SCM), was utilized. • Collected exact time and date of: • Order for feeding tube placement. • Order which states, “feeding tube – okay to use.” • X-ray confirmation performed first. • Order for tube feeding product.
Data Analysis • Literature review to determine average times for NSDs currently placing tubes. • Compared times to UK Hospital’s average time for tube placement. • Flowcharts • UK Hospital’s process • Process of other facilities
Results • Average time to establish enteral access and have tube cleared for use: • 16 hours 26 minutes. • Minimum = 3 hours 12 minutes. • Maximum = 37 hours 49 minutes. • No data gathered on how many attempts at placement.
Results • Average time to begin the feeding regimen once the tube was approved for safe use by the physician: • 8 hours 1 minute. • Maximum = 53 hours 1 minute. • Minimum = zero minutes. • 17 of 25 patients (68%) were ordered a tube feeding regimen within 15 minutes of the feeding tube being cleared for use.
Limitations • Small study sample. • No data collected on number of attempts at tube placement. • No data collected on total time for tube placement after admit to the ICU.
Comparison to Other Facilities • Medical College of Georgia (Cresci, 2003):
Conclusion and Recommendations • Tube placement is taking on average greater than 16 hours at UK Hospital. • The Gustafson Change Model (GCM) was utilized to examine the need for a change.
Recommendations • UK Hospital should closely evaluate the practice of NSDs placing bedside feeding tubes. • If the process change is implemented the following are suggested based on the GCM. • Implement a training program. • Develop a pilot program. • Hire an additional member to the nutrition support team. • Provide an in-service to critical care physicians regarding the change and its significance.
Recommendation 1 • Implement a training program. • Recruit one ICU nurse to serve as a mentor to train the NSD. • Create a competency checklist.
Recommendation 2 • Develop a pilot program. • Initially in one ICU. • Ideally in the same ICU as the nurse mentor. • Collect feedback to determine if the pilot should be expanded or if troubleshooting needs to take place.
Recommendation 3 • Hire an additional member to the nutrition support team. • Only if the pilot program is a success. • Ideally hire a dietitian. • Lower salary. • Team-based approach.
Recommendation 4 • Provide an in-service to critical care physicians regarding the change and its significance. • A recent journal article reported: • There is a “substantial discordance in physician perceptions and practice patterns regarding initiation and management of nutrition in ICU patients (Behara, 2008).”
Benefits of Reassigning Duty to NSDs • Nursing staff will be able to spend time on other patient-focused tasks. • NSDs will be given more responsibility. • Greater job satisfaction. • Increased recognition for dietetic profession due to advanced practice skills. • Patient will likely receive a higher quality of nutritional care in a more time efficient manner.
Special Thanks to My Capstone Committee Chair: Sarah Wackerbarth, PhD Second Member: Martha Riddell, DrPH Clinician: Beverly Lenahan, MS, RD, LD Reader: Dwight Denison, PhD