Download
1 / 124
1.26k likes | 1.71k Views
MS Patient Cases Iran May 2007. Jack Burks, MD Clinical Professor, Neurologist University of Nevada School of Medicine Reno, Nevada Vice President/Chief Medical Officer Multiple Sclerosis Association of America President Multiple Sclerosis Alliance.

E N D
MS Patient CasesIranMay 2007 Jack Burks, MD Clinical Professor, NeurologistUniversity of Nevada School of MedicineReno, Nevada Vice President/Chief Medical Officer Multiple Sclerosis Association of America President Multiple Sclerosis Alliance
Important Issues in Treating MS: Illustrative Patient Cases • When to start therapy? • How to decide on which therapy is the most effective for a specific patient? • How should patients be monitored to determine good/poor Rx. responses? • What is a poor response to treatment and how should it be managed? • How are side effects best managed? • What is the future for current and emerging therapies?
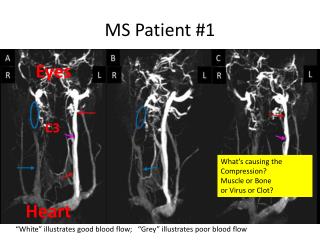
Patient 1:Deciding When to Initiate Treatment • History • 26-year-old secretary, mother of twins; no history of MS or SLE • Over 5-day period notices double vision, weakness in the right arm and leg, unsteady gait, fatigue, and difficulty with memory when multitasking • Exam • Diplopia on right gaze, mild right hemiparesis, and wide-based, slightly ataxic gait • Normal bedside mental status • Husband stresses patient’s recent disorganization
Patient 1: Deciding When to Initiate Treatment • MRI • 6 periventricular lesions, 1 pontine lesion, 1 high cervical lesion on T2 MRI • 4 GAD+ lesions • Lab work • All negative • Spinal tap not done
Neurologist’s Assessment • Patient had a CIS but does not meet the criteria for CDMS, could be ADEM • Steroids should be used in this patient, but a DMT is not appropriate at this stage • Is this the appropriate diagnosis? • What goes into the decision process to determine the appropriateness of utilizing a DMT?
Treat Early! Diagnosis of MSin Clinical Isolated Syndrome (CIS) Lesions in Time and Space Clinical Presentation Space Time (Add’l Requirements) (Add’l Requirements) 2 attacks; 2 locations No No 2 attacks; 1 location MRI abnormal or No 2 MRI lesions + CSF 1 attack; 2 locations No MRI 3 months or second attack 1 attack; 1 location (CIS) MRI abnormal or MRI 3 months 2 MRI lesions + CSF or second attack Ref: McDonald, I. Annals of Neurology 2002
McDonald MRI Criteria for Dissemination in Time • First scan 3 months after clinical event • New Gadolinium lesion • Must not be the same site • No new Gadolinium lesion: • Repeat MRI at ≥3 months • New T2 or gadolinium lesion The exact relationship between MRI findings and clinical status of patients is not completely understood. McDonald WI et al. Ann Neurol. 2001;50:121-127.
T2 3 months Gd Example Application of New Diagnostic Criteria .
Polman Revision of McDonald Criteria (2005) • New T-2 MRI lesions at 1 month after CIS MRI (lesions in time) • Spinal cord lesions can be considered as a brain infratentorial and, if Gd-enhancing, can substitute for a brain Gd-enhancing lesion Polman CH et al. Ann Neurol. 2005;58:840-846.
Patient 1: Follow-up • After being treated with a course of IV Solu-Medrol, the patient’s symptoms improved • At a 3-month follow-up visit: • Clinical signs resolved • Fatigue and memory problems less • Neurology exam normal • Previous GAD+ lesions had resolved • 1 new GAD+ lesion and 2 new T2 lesions
Neurologist’s Assessment at Follow-up • Patient meets the McDonald criteria for CDMS/RRMS • The patient was started on treatment • Do you agree with decision to treat? • How do you decide which DMT to utilize in this situation? • Is there a difference or are they all the same? • What do Evidence Based Medicine Analysis and Class I Head to Head Trial indicate?
Patient was treated with IFNβ-1b • BENEFIT Trial • 17 year follow-up data • AAN Treatment Guidelines
II. BENEFIT: Betaferon in CIS • Objective: • To assess efficacy, safety, and tolerability of every-other-day (EOD) interferon beta-1b treatment in patients with a clinically isolated syndrome (CIS) suggestive of multiple sclerosis • Study design: • Randomized, double-blind, placebo-controlled, parallel-group, multicenter study with 468 patients • Participants had experienced a first clinical demyelinating event, and at least 2 clinically significant MRI-detected brain lesions • Patients received Betaferon 250 µg or placebo SC EOD for 24 months or until CDMS • Primary endpoints: • Time to CDMS according to the modified Poser criteria • Time to diagnosis of MS according to McDonald diagnostic criteria Kappos L, Polman CH, Freedman MS, et al, for the BENEFIT Study Group. Treatment with interferon beta-1b delays conversion to clinically definite and McDonald MS in patients with clinically isolated syndromes. Neurology. 2006;67:1242-1249.
Design of the BENEFIT study Kappos L, Polman CH, Freedman MS, et al, for the BENEFIT Study Group. Treatment with interferon beta-1b delays conversion to clinically definite and McDonald MS in patients with clinically isolated syndromes. Neurology. 2006;67:1242-1249.
Betaferon Reduced the Risk of CDMSby clinical criteria 45% p<0.0001 Placebo Risk reduction* of 50% over 2 years(Hazard ratio= 0.5) 28% Clinically Definite MS (%) Betaferon *by adjusted proportional hazards regression days
+ 363 days: + 142% 25% Day 618 Day 255 Betaferon Delayed the Onset of CDMS 45% Placebo 28% Clinically Definite MS (%) Betaferon days
51% MRI MRI MRI MRI MRI MRI MRI Most Patients Develop MS by MRI Criteria Within 2 Years 85% Placebo McDonald MS (%) days The BENEFIT Study Group
Betaferon Doubles the Probability of Not Developing MS • Cumulative probability for patients not to develop MS according to McDonald Criteria over 2 years P<0.00001 2 x Cumulative probability Placebo (n= 176) Betaferon (n= 292) The BENEFIT Study Group
BENEFIT Trial: Early vs. Delayed Treatment: 3 year follow-up (2007) • Confirmed Progression (EDSS) • Placebo then Betaferon 24% • Betaferon from CIS 16% • 40% decrease of confirmed progression with early Betaferon treatment! (P=0.02) • No effect of NAbs on clinical outcomes
BENEFIT study: Discontinuation rates • Only 2.7% of Betaferon patients discontinued due to adverse events* • The majority of patients experienced no flu-like symptoms over 2 years Factors for low rate of discontinuation include: • Dosage Titration • Analgesics: before injection *From an analysis of patients who adhere to study protocol. The BENEFIT Study. Betaferon® in newly emerging multiple sclerosis for initial treatment: Clinical results [poster].
Lessons from BENEFIT Trial • Placebo patients studied in BENEFIT had a high risk of progressing to MS according to the McDonald criteria • 85% within 2 years, 51% after 6 months • In the BENEFIT study, every-other-day Betaferon significantly • Reduced the risk of progression to CDMS (by 50%) • Prolonged the time to CDMS by 1 year (+142%) (based on the 25th percentiles) • Delayed EDSS disability scores at 3 years • Every-other-day Betaferon is well tolerated and well accepted in patients
17 year follow-up Rationale • IFNB-1b was approved for the treatment of relapsing forms of multiple sclerosis (MS) based on the results of a double-blind placebo-controlled study in which patients received placebo or IFNB-1b for 104 weeks and were followed up for up to 5 years • Results of this pivotal study showed IFNB-1b to be effective and well tolerated over this period • There are few data regarding the long-term benefit of IFNB treatment for more than 10 years. However, given that MS evolves over several decades, there is a need for longer-term data on treatment outcomes • This study assessed the long-term impact of IFNB-1b therapy in patients involved in the pivotal study Ebers, George 2007
Credibility factors in Betaferon 17 year follow-up data • Positive: • Independent analysis • Intent to treat analysis: treated vs. placebo • About 90% case ascertainment • Betaferon effective and safe for 17 years • Concerns: • Unknown treatment modalities for some patients after trial ended • High rate of mortality in placebo group after trial ended. Is untreated MS a potentially fatal disease?
Long-term follow-up study:Betaferon significantly delayed disease progression over 17 years of treatment • Patients who continuously used Betaferon had nearly 60% more cane-free years from time of diagnosis* • Treatment with Betaferon delayed progression to SPMS by 6.6 years compared to other treatments or no treatment • After 17 years, the tolerability and safety profile of Betaferon remains excellent *Versus patients on other DMTs or no treatment. Goodin DS, Ebers G, Traboulsee A, et al, for the Betaferon® LTF Study group [poster]. American Neurological Association. October 8-11, 2006. Ebers G, Traboulsee A, Langdon D, Goodin D, Konieczny A, for the Betaferon®/Betaferon® LTF Study Group [poster]. American Academy of Neurology. April 1-8, 2006.
Betaferon 17-Year LTF:Mortality Data by treatment group • Betaferon standard dose (n=124) 6% • Betaferon lower dose (n=125) 9% • Placebo (n=123) 19%
Using Evidenced Based Medicine to Guide MS Therapy • AAN Guidelines • Cochrane Committee Reports • Head to Head Class I Trials
Evidence-based Medicine: AAN Guidelines Goodin DS, et al. Neurology. 2002;58:169-178.
AAN Guidelines on DMT’s • Relapses and MRI • All better than placebo (A) • Disability Progression • Interferons: Probably Effective (B) • Copaxone: Possibly Effective (C) • IFNs: Higher Dose / frequency more effective (B) • NAb: Conflicting data (U) • Utility of measuring is uncertain • Did not recommend testing requirements
Patient 2:Evaluating the Response to Disease Modifying Therapy (DMT) in MS
Patient 2: Evaluating Response to DMT • Current complaint • 28-year-old surgical resident with RRMS • Recently developed fatigue and frustration but without impairment of surgical skills, even during extended operations • She is considering changing her MS therapy
Patient 2: Evaluating Response to DMT (Cont.) • Past Neurological History • 3.5 yrs ago: first symptom (unsteadiness of gait) resolved without treatment or evaluation • 3 years ago: bladder urgency, difficulty handwriting, mild weakness in right leg • Brain MRI revealed 2 GAD+ lesions and 10 T2 lesions: locations included periventricular areas, brain stem, cerebellum and corpus Callosum. • CSF: + bands and IgG Synthesis: Other labs normal • Diagnosis of RRMS was made and treatment was I.V. Steroids for 5 days. IFN B-1b was also begun. She recovered completely in one month • 6 months later: mild blurred vision in left eye for two weeks with spontaneous recovery without steroids. No Evaluation
Patient 2: Evaluating Response to DMT (Cont.) • Current evaluation: • Neuro Exam Normal: Possible depression? • MRI: No GAD lesions: T2 lesions are smaller. No black holes or atrophy • NAb test: + (1:100 titer)
Neurologists Assessment • Since IFN B-1b, this patient has had only one episode of (likely) mild optic neuritis – shortly after beginning therapy 3 yrs ago • Neuro exam was normal • MRI demonstrated improvement since beginning therapy • Patient does not have enough evidence to diagnose “suboptimal response” to current therapy.
Neurologist’s Action Plan • Patient should remain on IFN B-1b • Treat symptomatically for fatigue & depression • Patient and NAb status should be reevaluated in 6 months
Questions • What is the utility of NAb testing in this clinically stable patient? • What will be the patient’s response to changing a treatment that is apparently working, especially if the change results in a treatment that may not work as well?
Comments • There remain differences of opinion regarding the use NAb testing. 2007 AAN guidelines using EBM principles do not support routine NAb testing because • No class I EBM results on utility of NAb testing • No standardized NAb test • No established level of NAb relevance (?100-200) titer • No EBM data on timing of NAb test • No EBM data on clinical outcomes after changing therapy based on + NAb test • Recent data fails to correlate NAbs with poor response to treatment.
Neutralizing Antibodies to Interferon B-1b are not Associated with Disease Worsening in Multiple Sclerosis Goodin DS., Hurwitz B., Noronha A. The Journal of International Medical Research, 2007; 35: 173-187
NAb Results:6698 Patients • Australia: All Patients on IFNβ-1b • 37% NAb positive • North America: Suboptimal Responders • 21.3 % NAb positive • Europe: Suboptimal Responders • 27.6% NAb positive Goodin, 2007
Conclusions: • Poor responders were less likely to have NAbs than responders • NAbs are not responsible for poor clinical responses and that NAb status is of little clinical value. Goodin DS., Hurwitz B., Noronha A. The Journal of International Medical Research, 2007; 35: 173-187
Evaluating Response to DMT: Patient 2 Follow-up • 6 months later she was NAb Θ on retest • The patient has remained on IFN B-1b with no new symptoms for the last 2 years • Modafinil was added for fatigue: improvement • SSRI taken for depression for one year. • She is now a fully functioning surgeon with no depression and minimal fatigue
Patient 4: Managing Side Effects of DMT’s • 34 yr old RRMS patient has been on IFN B-1b for 4 months • Neurologically stable but experiences flu like side effects and redness/pain at injection sites. She is unable to work because she feels “sick”, agitated, and depressed. Although feeling better in the past 2 months, she still wants to stop or switch treatment. • Initially she was started on the full dose of IFN B-1b without titration or analgesia pre-injection medication. Her husband has been injecting the drugs at an angle “to avoid going too deep”. • Liver function and CBC tests are normal • MRI is unchanged
Neurologist’s Assessment • Since beginning therapy she has had no relapses or new MRI lesions • Side effects are caused by lack of dose titration when starting treatment and improper injection technique (Intradermal injections). • Depression could be from learning of her diagnosis of MS or worry about drug side effects vs. a direct effect from drug.
Neurologist’s Actions • Drug holiday for one month • Re-start IFN B-1b at ¼ dose and titrate to ½, then ¾ and then full dose each 2-3 weeks • Close supervision and counseling • Take analgesics before each shot • Inject at 90 degrees • Evaluate for depression on each visit, but no anti depression medication at this time
Patient 4: Outcome • At 1 year patient tolerated treatment well with very few side effects and no recurrence of depression symptoms. • No missed days from work
Patient : Discussion • Drug side effects may mimic worsening of MS • Proper initiation of therapy prevents most early side effects • Aggressive side effect management can often avoid terminating therapy
Patient 5: Deciding When Treatment Is Not Working • A 43-year-old patient seeks a second opinion • 5-year history MS • Treated for 3 years with IFNβ-1a IM weekly • Clinical exam • Weakness in extremities (worst in left lower) • Uses cane for balance (4 months) • Bilateral extensor plantar responses • decreased vibration and position sensation in both legs and left hand • Dysmetria bilaterally on finger to nose, and rapid alternating movements bilaterally; dysmetria on heel to shin • Mild memory dysfunction
Patient 5: Summary of Disease Course • A 43 yr old salesman is referred to you for a second opinion • Case history