Download
1 / 52
980 likes | 3.29k Views
The Male Breast. M.Sklair -Levy, M.D Radiology Department Sheba Medical Center Israel. The Male Breast . Clinical symptoms Unilateral, bilateral breast enlargement Breast pain Breast lump Most of the evaluated lesions are benign Most related to gynecomastia. Introduction .

E N D
The Male Breast M.Sklair-Levy, M.D Radiology Department Sheba Medical Center Israel
The Male Breast • Clinical symptoms • Unilateral, bilateral breast enlargement • Breast pain • Breast lump • Most of the evaluated lesions are benign • Most related to gynecomastia
Introduction • Male breast carcinoma is a rare disease • < 1% of all malignancies in men • 1% of all breast cancers
Introduction • Clinically suspicious lesions • Imaging evaluation • Mammography • US - In patients with questionable findings at mammography and for lesions that are difficult to image with mammography • The relationship of the mass to the nipple should be carefully assessed • an eccentric location is highly suspicious for cancer.
Breast Development • The breast tissues of both sexes are identical at birth • Estrogen stimulates breast tissue • Androgen antagonizes these effects • At puberty in boys - increase in estrogen,testosterone • Transient proliferation of the ducts and stroma • Followed by involution and ultimate atrophy of the ducts.
Characterized: Subcutaneous fat Remnant of subareolar ductal tissue Lobular development - which requires both estrogen and progesterone, is usually not observed in men Normal Male Breast
Normal Male Breast - US Anatomy of the normal male breast- consists of the skin and subcutaneous fat. The pectoralis fascia (PF), pectoralis muscle (PM), ribs,and intercostal muscles (ICM)
Introduction • The two most important disease of the male breast • Gynecomastia • Breast cancer • The majority of lesions in male breasts are benign • Other disease arise from the skin&subcutan. • Fat necrosis • Lipoma • Epidermal inclusion cyst
Imaging of the Male Breast • Mammography - diagnose gynecomastia and breast carcinoma • Diagnostic mammography • Standard mammographic views - CC & MLO • Magnification and spot compression views • US- suspicious findings on mammography • effective for evaluating male patient as it is for female
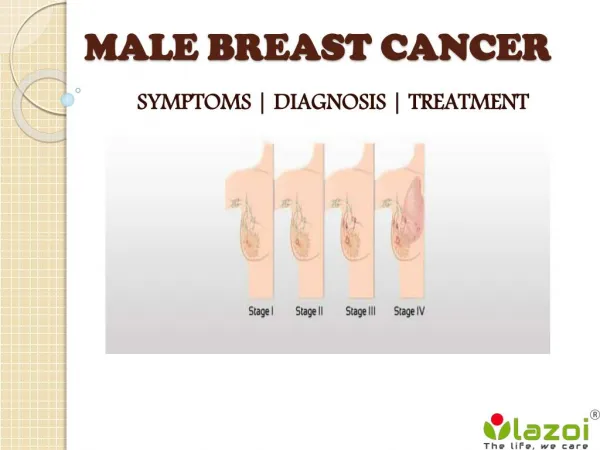
Male Breast Cancer • Male breast cancer - uncommon • less than 1% of all malignancies in men • only 1% of all breast cancers • The mean age of diagnosis is 67 years • Less than 6% of cases occur in males under the age of 40 years.
Male Breast Cancer Risk factors • advanced age • prior irradiation of the chest • exogenous estrogen for prostate cancer treatment • gender-reassignment procedures • liver disease and other diseases associated with hyperestrogenism, androgen deficiency due to testicular dysfunction • genetic and chromosomal conditions - BRCA2 , Klinefelter syndrome
Male Breast Cancer • Clinical manifestation– hard , fixed , painless mass • Bloody nipple discharge common • Secondary signs occur earlier in male patients because of smaller breast size. • nipple retraction, skin ulceration,thickening,increased breast trabeculation • Palpable axillary lymph nodes are present in about 50% of cases
Male Breast Cancer • Diagnostic work-up: • Bilateral Mammography • US • Biopsy • Staging and treatment are similar to those of female breast cancer
Male Breast Cancer • Histologic subtype : • Invasive ductul carcinoma- most common – 85% • Ductal carcinoma in situ • Male breast contains only ducts • Invasive lobular – rare – • No lobules formation in male breast
Male Breast Cancer • Treatment • Same as for women • Surgery • Axillary node dissection • Chemotherapy • Radiation therapy • Prognosis identical
Male Breast Cancer- Mammographic Appearance • Location - Subareolar position , eccentric to the nipple • Margins– well-defined, ill-defined, spiculated • Shape– round, oval, irregular , lobulated • Calcification– few , coarser • Secondary signs– skin thickening, nipple retraction , axillary lymphadenopathy
US Features-Male Breast Cancer • Male breast cancers have similar US features as in women • Masses - nonparallel, discrete, hypoechoic. • Margins - angulated , microlobulated, or spiculated • Microcalcification - punctate high echogenicity • Posterior acoustic features are not helpful for distinguishing benign versus malignant lesions • no posterior acoustic feature • posterior enhancement • posterior acoustic shadowing
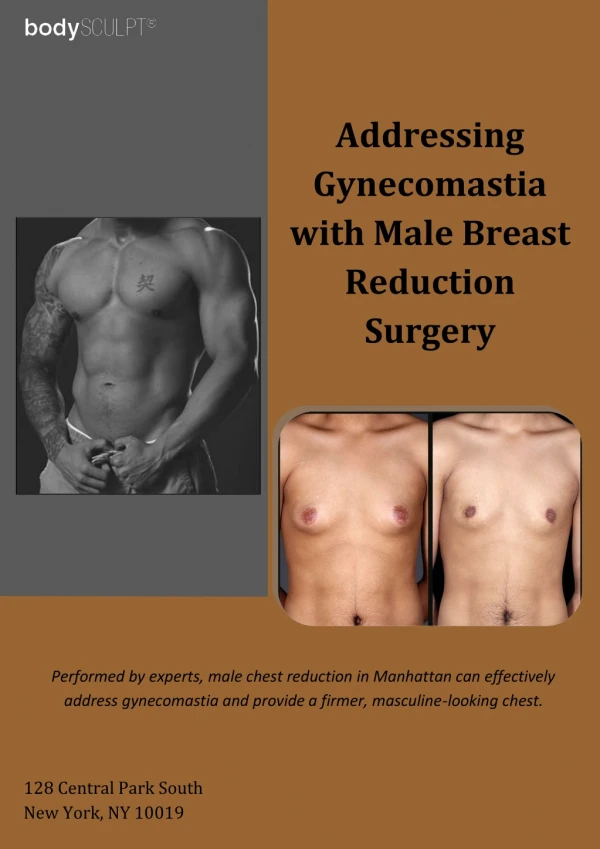
Benign Mimics of Male Breast Cancer Gynecomastia
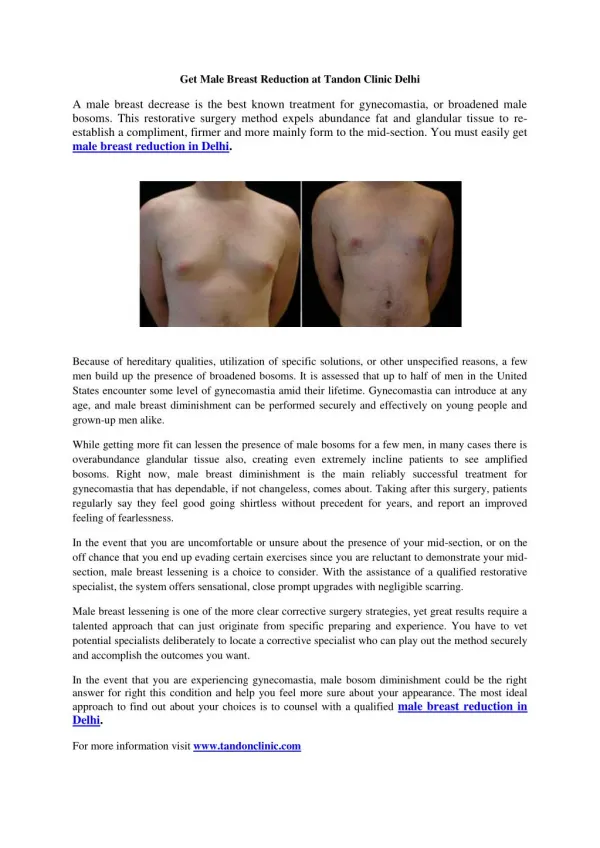
Gynecomastia • Gynecomastia is the most common benign condition of the male breast • It is enlargement of the male breast due to benign ductal and stromal proliferation. • Causes breast enlargement /subareolar mass with/without associated breast pain • It can be unilateral, bilateral symmetric, or bilateral asymmetric.
Gynecomastia • The hallmark of gynecomastia is its central symmetric location under the nipple • Reversible in early stages– if the cause is corrected • Reversible phase progress to late periductal edema with irreversible stromal fibrosis
Gynecomastia • Associated with increased levels of estradiol and decreased levels of testosterone • Physiologic changes at puberty senescence • Endocrine and hormonal disorders • Systemic disease • Neoplasm • Drugs
Physiologic Senescence Puberty Hormonal Klinefelter syn Hypogonadism Systemic disease Cirrhosis Chronic renal insufficiency Idiopathic Neoplasm Adrenal carcinoma Pituitary adenoma Hepatocellular carcinoma Drug use Cimetidine Marijuana Thiaside diuretics Omeprazole Tricyclic antidepresasants Spironolactone Diazepam Anabolic steroids Exogenouis estrogen Causes of Gynecomastia
Gynecomastia • 3- mammographic patterns -representing various degrees and stages of ductal and stromal proliferation • Nodular • Dendritic • Diffuse glandular
Gynecomastia • Nodular G.- most common–77% • Pathology– florid g. –early phase • patients with gynecomastia < 1year • The majority of patients will present with • nipple tenderness , palpable lump • Mammography-nodular subareolar density • The typical mammographic confirms the diagnosis and requires no further imaging work-up.
Mammography - Nodular G. Nodular subareolar density
Nodular G • US- a subareolar fan- or disk-shaped hypoechoic nodule surrounded by normal fatty tissue • The zone of transition may be poorly defined, with lobular margin • Hypervascularity can be seen secondary to stromal proliferation • US - In cases of equivocal clinical and mammographic findings • follow-up evaluation
US - Early Nodular Gynecomastia Hypervascular flow within the mass subareolar, fanshaped,hypoechoic nodule surrounded by echogenic normal fatty tissue
Chronic Dendritic Dynecomastia • Chronic dendritic gynecomastia (quiescent phase) -20% • Patients with gynecomastia > 1 year. • Pathology–fibrous g.- long standing gynecomastia • Fibrosis becomes the dominant process and is irreversible. • Mammography - dendritic subareolar density with posterior linear projections radiating into the surrounding tissue toward the uoq
Mammography - Chronic Dendritic G. Dendritic subareolar density with posterior linear projections radiating into the surrounding tissue
Chronic Dendritic Gynecomastia • US- a subareolar hypoechoic star-shaped, fingerlike projections or “spider legs” • benignity - directly from the undersurface of the nipple without causing any overlying skin thickening or nipple retraction.
US- Chronic Dendritic Gynecomastia US- subareolar hypoechoic nodule with star-shaped projections into the surrounding echogenic fibrous tissue
Chronic Dendritic Gynecomastia • The clinical history, particularly the duration of symptoms, can also be helpful in making this diagnosis. • patients may have an acute episode of gynecomastia in addition to chronic dendritic gynecomastia. • both phases can be seen at imaging simultaneously.
Diffuse Glandular Gynecomastia • Diffuse glandular–3% • Patients receiving exogenous estrogen • Mammography- enlargement of the breast , similar to heterogeneously dense female breast • Irreversible stromal fibrosis and ductal epithelial atrophy develop, the breast enlargement may decrease but not completely resolve.
Diffuse Glandular Gynecomastia Enlargement of the breast and diffuse density with both dendritic and nodular features
Diffuse Glandular Gynecomastia • US - both nodular and dendritic features are seen surrounded by diffuse hyperechoic fibrous breast tissue
Diffuse Glandular Gynecomastia Heterogeneous breast with both nodular and dendritic projections surrounded by diffuse hyperechoic fibrous tissue.
Pseudogynecomastia • Pseudogynecomastia – a fatty proliferation of the breasts , without proliferation of glandular tissue. • Difficult to distinguish from normal male breast on mammography • Diagnosis requires clinical correlation with breast enlargement
Less Common Benign Conditions • Lipoma - second most common benign lesion in the male breast • Mammography typically shows a subtle encapsulated fatty mass in the palpated area • US - demonstrates one or multiple parallel, homogeneous, and mildly hyperechoic masses under the skin • capsule is sometimes seen
Lipoma Parallel, homogeneous, mildly hyperechoic mass with a capsule (arrow) under the skin. Subtle encapsulated fatty mass (arrows) in the palpated region.
Epidermal Inclusion Cyst • Epidermal inclusion cyst is the third most common benign lesion in the male breast • Arise from obstructed or occluded hair follicles, at the sites of previous skin trauma such as a surgical wound or insect bites • Composed of laminated keratin surrounded by stratified squamous epithelium
Epidermal Inclusion Cyst • Mammography- well-defined dense oval mass contiguous with the skin in the palpable area • US- hypoechoic lesion that is contiguous with the epidermis, the claw sign , with increased through transmission. • This feature is the key to distinguishing this benign condition from cystic malignancies of the male breast.
Epidermal Inclusion Cyst Hypoechoic lesion, which is contiguous to the epidermis (arrows) (the “claw sign”) with increased through transmission well defined, dense, oval mass contiguous to the skin in the palpated region.
Benign ConditionsAssociated with Gynecomastia • Pseudoangiomatous stromal hyperplasia (PASH)- benign stromal tumor formed by myofibroblasts and with glandular hyperplasia • Often incidentally seen in gynecomastia • Mammography- noncalcified breast mass, circumscribed or partially circumscribed • US - solid circumscribed hyperechoic masses • Recurrence is common after resection
PASH Solid hyperechoic mass with posterior acoustic shadowing Dense circumscribed mass
Intraductal Papilloma • Intraductal papilloma - benign proliferation of intraductal mammary epithelium. • Mammography - discrete dense mass against a background of subareolar changes consistent with gynecomastia • US– multiple eccentric, subareolar, elongated and welldefined hypoechoic masses, which have irregular shapes and are possibly confined to the lumina of markedly enlarged central ducts • cystic areas - represent associated ductal ectasia
Intraductal papilloma US-multiple eccentric, subareolar, elongated,well-defined, hypoechoic masses ;US image shows cystic areas, which may represent associated ductal ectasia. discrete dense mass against a background of subareolar density, which consistent with gynecomastia
Conclusions • The majority (99%) of male breast lesions are benign • Mammography- for clinically suspicious lesions • accurate for diagnosing gynecomastia • US useful for further characterization • The relationship of the mass to the nipple should be carefully assessed • Eccentric location is highly suspicious for cancer • US of the axillary region is helpful for staging