Download
1 / 19
2.55k likes | 7.38k Views
Jaundice . http://thestandard.org.nz/wp-content/uploads/2010/09/Dr-Nick-Riviera.png. Steven Smith. Objectives. Bilirubin Physiology Jaundice Definitions Jaundice Presentation History and examination Investigations & Interpretation Differential Diagnosis Approach to differential

E N D
Jaundice http://thestandard.org.nz/wp-content/uploads/2010/09/Dr-Nick-Riviera.png Steven Smith
Objectives • Bilirubin Physiology • Jaundice Definitions • Jaundice Presentation • History and examination • Investigations & Interpretation • Differential Diagnosis • Approach to differential • Key diagnoses
Bilirubin Metabolism Longmore M. Wilkinson I. Turmezei T. Cheung CK. Oxford Handbook of Clinical Medicine 8th edition
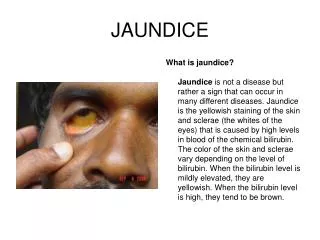
Jaundice • Yellow pigmentation of the skin, sclerae and mucosae • Caused by excess circulating bilirubin • Normal serum bilirubin is 3 to 17 μmol/L • Detectable clinically when serum bilirubin is greater than 35μmolL-1
Some Definitions • Prehepatic - excessive production of bilirubin • Hepatic - Pathology within hepatocytes • Post hepatic - Problem with biliary flow • Conjugated (direct)- Accumulation of conjugated bilirubin • Unconjugated (indirect)- Accumulation of unconjugated bilirubin • Obstructive - Lack of bile flow
http://en.wikipedia.org/wiki/File:Jaundice08.jpg Patient presenting with jaundice
History • Presenting complaint • Acute or chronic • Associated features • Pain (RUQ), Nausea +/- vomiting, Puritis (itch), Fever, Dark Urine, Diarhoea, Steatorrhoea, Weight loss, Night sweats, Loss of Appetite • Past medical History • Gallstones, Liver disease, Haemophilia, Recent transfusion, Ulcerative Colitis, Diabetes Mellitus, Emphysema • (Psychosis)
History • Medications (including OTC & herbal) • Haemolysis • Cephalosporins – 3rd generation • penicillin • aspirin • Hepatitis • Paracetamol overdose • Rifampacin, isoniazid • Cholestasis • Antibiotics: beta-lactams (flucloxacillin) • Chlorpromazine
History • Social History • Alcohol consumption – units per week • IVDU • Unprotected sex/multiple partners • Foreign travel – malaria, hep A or E • Tattoos • Ethnic background & country of birth • Sickle cell • Thalassaemia & G-6-PDH deficiency • Family History • Jaundice, Liver disease, cancer or haemolytic anaemia.
Examination • Signs of: • Chronic liver disease • Haemolysis • Biliary obstruction • Features indicative of specific disease • Kayser-Fleisher rings in iris • Bronzed tan • Cachexia • Murphy’s Sign
Investigations • 1st Line • Bloods - FBC, LFT’s, U+E’s, Clotting, Amylase • Urinalysis – bilirubin • 2nd Line • Imaging – USS • Further Bloods - Blood film, Viral Serology Autoimmune screen, Ferritin and transferrin, Cu and Caeruloplasmin • 3rd Line • MRCP/ERCP • Liver biopsy – USS or CT guided
Bloods – Liver enzymes • Bilirubin levels • Confirm hyperbilirubinaemia • >20% bilirubin conjugated – suggests obstruction to flow • ALT and AST • Raised if there is damage to hepatocytes • Normal level in serum = <40U/L • Very high in acute hepatocellular damage/necrosis • 8-20 fold above normal (ALT>AST) • Milder rise in chronic liver disease or extrahepatic obstruction • Alkaline Phosphatase and γ-GT • Released from damage to biliary epithelial cells • Alk phos also from bones with high turnover and placenta • γ-GT almost exclusive to biliary cells
An Overview Differential Diagnosis http://www.flickr.com/photos/jeffpro/5084387279/
Differential Diagnosis • 3 main problems • Increased bilirubin production • Intravascular haemolysis • Extravascular haemolysis • Decreased conjugation • Reduced hepatocyte uptake • Enzymatic problems • Decreased excretion • Can’t be excreted into bile canaliculi • Can’t pass through biliary tree Unconjugated Conjugated
http://i102.photobucket.com/albums/m83/lavopal/Jaundice-Hulk.jpghttp://i102.photobucket.com/albums/m83/lavopal/Jaundice-Hulk.jpg
References • Oxford handbook Clinical Medicine • Oxford handbook for the foundation programme • Oxford cases in medicine and Surgery • Kumar and Clark • BMJ Best Practice