Download
1 / 14
140 likes | 292 Views
Community Care of North Carolina (CCNC). CHIPRA A Quality Demonstration Grant

E N D
Community Care of North Carolina (CCNC) CHIPRA A Quality Demonstration Grant CHIPRA Team: *Marian Earls, MD, *James Green, Data Analyst, *Stacy Warren, Project Director, *Kern Eason, Central PEHR Consultant, *Janie Shivar, Category A Clinical Consultant, Maria Dover, Connect Clinical Consultant, *Marla Satterfield, Connect Clinical Consultant Key Partners: NC Chapter of the AAP, American Academy of Family Physicians, Center of Excellence for Integrated Care, & the Oral Health Division of DMA
CHIPRA Categories A - Experiment with and evaluate the use of new and existing measures of quality for children B – promote the use of health information technology (HIT) for the delivery of care for children C – evaluate provider-based models to improve the delivery of care D – demonstrate the impact of model pediatric EHRs (electronic health records) E – creating targeted models to demonstrate their impact on health, quality and cost.
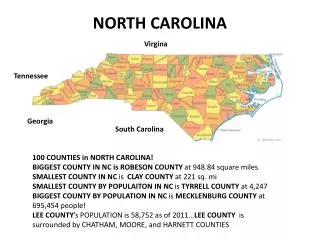
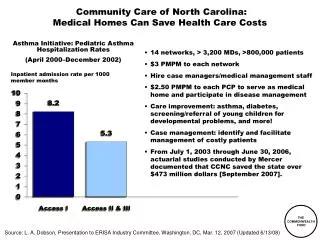
Community Care of North Carolina (CCNC)Why is it Unique? CCNC is made up of 14 Networks which represent all 100 NC counties. CCNC has created an infrastructure that is data driven. Over 90% of NC’s primary care providers belong to a CCNC network. CCNC believes in doctors working with other doctors to improve quality and decrease costs of healthcare. Camden Alleghany Currituck Northhampton r Gates Warren Ashe Surry Stokes a Person Rockingham Caswell Vance Pasquatank Hertford Halifax Watauga Perquimans Wilkes Chowan Yadkin Granville Avery Forsyth Bertie Franklin Orange Guilford Mitchell Alamance Durham Caldwell Alexander Nash Tyrrell Davie Yancey Edgecombe Madison Wake Washington Dare Iredell Davidson Martin Burke Wilson Randolph Chatham McDowell Catawba Buncombe Rowan Pitt Beaufort Haywood Hyde Swain Johnston Lincoln Rutherford Lee Greene Graham Henderson Cabarrus Harnett Jackson Wayne Gaston Stanly Polk Moore Cleveland Lenoir Transylvania Montgomery Craven Cherokee Mecklenburg Macon Pamlico Clay Sampson Cumberland Jones Richmond Hoke Union Anson Duplin Scotland Carteret Onslow Robeson Bladen Pender New Columbus Hanover Brunswick
BreakthroughResults A P Evidence & Data S D A P S D A P S D A P Learning and improvement Theories, hunches,& best practices S D Categories A, C &DThe Quality Improvement Cycle PDSA Ramps Plan * Do * Study * Act
Category A - Core Quality Indicators 24 Quality Indicators NC Unique Indicators By the end of 2011 NC projects we will be able to report on 12 of the 24 measures By the end of 2012, NC projects we will be able to report on all of the 24 measures All 24 Quality Indicators will be reported to CMS annually Some of the 24 measures will be reported to the Networks and Practices quarterly in order to promote quality improvement initiatives‘ NC Unique measures to be reported on Quarterly • EPSDT Report Card • Dental Varnishing • Developmental & Behavioral Screening-all ages • Obesity • Foster kids linked to Medical Home • ABCD • ADHD quarterly measure - TBD CCNC believes that in order to ‘move the needle’ on improving healthcare, real time data needs to be given to practices consistently and timely so this information is meaningful and actionable.
CHIPRA C or CHIPRA ‘Connect’ • Promoting Medical Homeness • Implement Mental Health competencies in primary care by using the AAP Mental Health Toolkit • Promoting Routine Screens for children of all ages with special emphasis on: • Maternal Depression Screens • Autism Screens • School Age screens • Adolescent screens • Promoting primary care providers and community service providers ability to: • Build strong relationships • Communicate effectively • Collaborate to promote family centered care MoC-IV available to pediatricians and family physicians for QI projects including: Adolescent Screening, Maternal Depression Screening & Oral Health Screening.
Connect - Chart Extraction and Evaluation Monthly Chart audits are completed by QI specialists and auto populated into the chart extraction tool. Run chart data is analyzed and reported monthly. QI specialists amend PDSA projects according to data trends.
Category D – Project OverviewThe Pediatric EHR Format Existing EHR systems often do not optimally support the provision of health care to children. The goal is to develop a model EHR Format for children, demonstrate that it can be readily used, and package it in a way that facilitates broad incorporation into EHR systems. The elements of the EHR to be tested will be developed with practices input during the planning and infrastructure development phase. It is anticipated that the model will influence the criteria for future EHR product certification.
NC PEHR Survey of Gaps A March 2011 survey of NC pediatric practices identified the following gaps in current EHRs: Working with Westat and the AAP to identify additional gaps and to develop a model EHR, optimized for child health. Model Sample: • Asthma Severity Scoring • The system SHALL support Asthma Severity Scoring. • Documentation of pertinent family history • The system SHOULD incorporate documentation of pertinent family history to screen children at risk for common chronic conditions such as asthma and diabetes (Trotter & Martin, 2007) • Capture/calculate coded individualized disease measure goals and thresholds • The system SHOULD capture/calculate coded individualized disease measure goals and thresholds for modifying care (e.g. peak flow, FEV1, HgA1c, or behavioral goals used in self-care and inpatient treatment plans). CHIPRA Category-D
In North Carolina….. Children present a prime opportunity to prevent health issues from becoming chronic adult concerns. All 14 Networks will work with providers/medical homes interested in implementing the model EHR. We will be collaborating with the NC REC throughout this project. Next Steps Identify Vendors Identify Practices Evaluation Design Research
Evaluation Currently we are identifying vendors who wish to incorporate the model in their product offerings and are eager to help their clients/customers improve evidence-based care of children. Our longer-term evaluation plan will engage individual practices in measuring the effect of the Pediatric EHR model in changing the way care is delivered and received. Vendor #3 Vendor #1 Vendor #4 Vendor #2 CHIPRA Category-D
Measurement Possibilities Current Future Claims - Population level data but the scope is limited to billable items. Chart Extraction – Is able to gather more robust quality measures but scope is limited because it is only a small sample of the population With EHR adoption Data can be gathered on the broad population and provide information on how care was delivered.
Breadth and Depth PEHR Quality Measures Chart Claims Data Population
Integration of Categories A, C, and D Each strategy will propel quality improvement both independently and in concert with the other strategies EHR supports Medical Home implement quality care Measures inform and evaluate impact of EHR D Pediatric Electronic Health Record Medical Homes will drive service-oriented, quality EHR development Measures enable ongoing, flexible tracking of Medical Home Impact EHR enables will enable efficiencies and timely tracking and meaningful use of quality measures A Quality Measures Medical Homes provide data on feasibility, cost and value of measures C Medical Home