Download
1 / 33
330 likes | 349 Views
Early and Accurate Diagnosis of Idiopathic Pulmonary Fibrosis (IPF). Objective. Discuss the diagnostic strategies for facilitating early and accurate diagnosis for IPF (clinical, radiologic, and pathologic evaluations). Approach to Diagnosis of IPF. Clinical evaluation Radiologic evaluation

E N D
Early and Accurate Diagnosis of Idiopathic Pulmonary Fibrosis (IPF)
Objective Discuss the diagnostic strategies for facilitatingearly and accurate diagnosis for IPF (clinical,radiologic, and pathologic evaluations)
Approach to Diagnosis of IPF Clinical evaluation Radiologic evaluation Pathologic evaluation
Clinical Evaluation • Major criteria • Exclusion of other known causes of ILD • Abnormal pulmonary function tests that include evidence of restriction and impaired gas exchange • Bibasilar reticular abnormalities with minimal ground glass opacities on HRCT scan • Transbronchial lung biopsy or BAL without features to support an alternative diagnosis ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2002;165:277-304.
Clinical Evaluation • Minor criteria • Age > 50 yr • Insidious onset of otherwise unexplained dyspnea on exertion • Duration of illness > 3 mo • Bibasilar, inspiratory “Velcro-like” crackles All major criteria and at least 3 of the minor criteria must be present to increase the likelihood of an IPF diagnosis ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2002;165:277-304.
Pulmonary Function Tests • Typical findings in IPF patients: • Restriction • Reduced FVC and TLC • Normal or increased FEV1/FVC ratio • Impaired gas exchange • Decreased DLco, PaO2 • Desaturation on exercise oximetry • Increased A-a gradient • Normal resting PFTs do not exclude IPF ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2000;161:646-664.
6-Minute Walk Test for Interstitial Lung Disease • Baseline blood pressure, pulse, O2 saturation • Timed walk at any pace • As many stops as necessary • If oxygen saturation persistently less than 88%, repeat test with supplemental oxygen • Primary endpoint is walk distance Enright PL. Respir Care. 2003;48:783-785; ATS. Am J Respir Crit Care Med. 2002;166:111-117.
Desaturation on 6-Minute Walk Test • Desaturation may occur in several lung diseases • Interstitial lung diseases • Pulmonary hypertension • Severe obstructive lung disease • If desaturation occurs on 6MWT and an ILD is suspected, then HRCT may be indicated Enright PL. Respir Care. 2003;48:783-785; ATS. Am J Respir Crit Care Med. 2002;166:111-117.
Desaturation on 6MWT Predicts Decreased Survival in UIP (N = 83) Desaturators 1.0 69% 0.8 0.6 35% Survival Probability 0.4 P = 0.0018 Lama VN, et al. Am J Respir Crit Care Med. 2003;168:1084-1090. 0.2 0.0 0 2 1 3 4 5 Nondesaturators Years
Desaturation on 6MWT Predicts Decreased Survival in NSIP (N = 22) 100% 1.0 0.8 66% 0.6 Survival Probability 0.4 P = 0.0089 0.2 0.0 0 2 1 3 4 5 Nondesaturators Years Desaturators Lama VN, et al. Am J Respir Crit Care Med. 2003;168:1084-1090.
Differential Diagnosis • Other idiopathic interstitial pneumonias • NSIP • DIP • RBILD • AIP • COP • Connective tissue diseases • Scleroderma • Rheumatoid arthritis • Polymyositis/dermatomyositis • Asbestosis • Hypersensitivity pneumonitis • Sarcoidosis ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2000;161:646-664.
Diseases That Mimic IPF • IPF is often misdiagnosed, or diagnosed at an advanced stage of the disease • Symptoms of other diseases that mimic IPF: • COPD • CHF • Connective tissue diseases (eg, RA, Sjögren’s, SLE) • Other lung diseases (asbestosis, hypersensitivity pneumonitis) ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2000;161:646-664. ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2002;165:277-304.
Clinical Evaluation • Useful serology to exclude/include other diseases • ESR • ANA • RF • Scl-70 • CPK and aldolase • Jo-1 antibody • ANCA • ACE • Hypersensitivity panel (follow-up with exposure history) Adapted from ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2000;161:646-664.
Idiopathic Pulmonary Fibrosis (IPF)Chest X-Ray Findings • Reduced lung volume • Reticular opacities • Honeycombing sometimes visible • Lower-lobe and peripheral predominance of abnormalities • HRCT should be performed in all patients with suspected IPF, even if CXR is typical
Typical Features of IPF on Chest X-Ray Abnormal CXR Normal CXR Slide courtesy of Ganesh Raghu, MD.
High-Resolution CT Technique • Thin collimation (eg, 1 mm) • Spaced images (1–2 cm) at full inspiration • Volumetric helical HRCT may be used but results in a greater radiation dose • Additional prone scans often best for showing early abnormalities • Window mean -600 to -700 H • Window width 1000 to 1500 H Slide courtesy of W. Richard Webb, MD.
Idiopathic Pulmonary Fibrosis (IPF) HRCT Findings • Peripheral honeycombing • Irregular reticular opacities • Traction bronchiectasis • Minimal ground-glass opacity • Sub-pleural, posterior, lower-lobe predominance of abnormalities ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2000;161:646-664.
Early HRCT Findings in IPF Slide courtesy of Kevin O. Leslie, MD.
UIP: Honeycombing Slide courtesy of W. Richard Webb, MD.
UIP: MinimalHoneycombing Slide courtesy of W. Richard Webb, MD.
UIP: Irregular Reticular Opacities Slide courtesy of W. Richard Webb, MD.
UIP: Traction Bronchiectasis Slide courtesy of W. Richard Webb, MD.
Subpleural and Basal Predominance Slide courtesy of W. Richard Webb, MD.
HRCT Diagnosis of IPF • Prospective study of 91 patients with suspected IIP • 54 (59%) had IPF • 37 (41%) had other diseases • On HRCT, radiologists “certain” of dx in 52 (57%) of 91 • “Certain” IPF: diagnosis correct in 26 (96%) of 27 • “Certain” non-IPF: correct in 21 (84%) of 25 • Confident clinical/HRCT diagnosis of IPF: SLB probably unnecessary • Confident clinical/HRCT not IPF and diagnosis uncertain: SLB indicated Hunninghake et al. Am J Respir Crit Care Med 2001; 164:193-196.
HRCT Diagnosis of IPF • Independent predictors of IPF • Lower-lobe honeycombing (odds ratio 5.36; P = 0.007) • Upper-lobe reticular opacities (odds ratio 6.28; P = 0.004) • In patients presenting with a clinical syndrome suggestive of IIP, CT findings of lower-lung honeycombing and upper-lung irregular lines are most closely associated with a pathologic diagnosis of UIP Hunninghake et al. Chest 2003; 124:1215-1223.
HRCT Diagnosis of IPF Hunninghake et al. Chest 2003; 124:1215-1223.
HRCT Diagnosis of IPF • 73 patients with UIP; 23 with NSIP • Honeycombing on HRCT = definite or probable UIP • All 27 patients with a HRCT diagnosis of definite or probable UIP had UIP on biopsy • Patients with HRCT diagnosed definite or probable UIP had shortest survival Flaherty et al. Thorax. 2003;58:143-148.
Survival in Relation to HRCT and Histology Diagnostic Category Deaths/Patients (%) Median Survival (yrs) Histological Diagnosis UIP NSIP 34/73 (47) 2/23 (9) 3.98 > 9 HRCT Diagnosis Definite/probable UIP Indeterminate Definite/probable NSIP 17/27 (63) 9/25 (36) 10/44 (23) 2.08 5.76 5.81 Histological HRCT UIP UIP NSIP NSIP 17/27 (63) 17/46 (37) 2/18 (11) 0/5 (0) 2.08 5.76 > 9 > 6.6 Def/Prob UIP Def/Prob NSIP Def/Prob NSIP Indeterminate Table adapted from Flaherty KR, et al. Thorax. 2003;58(2):143-148.
Role of BAL vs Biopsy in IPF ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2000;161:646-664; 2002;165:277-304.
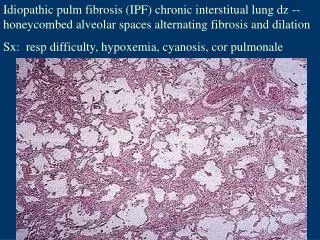
Diagnostic Pathologic Findings in UIP • UIP pattern • Fibroblastic foci • Temporal heterogeneity • Honeycombing • Minimal inflammation ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2000;161:646-664; 2002;165:277-304. .
Approach to Diagnosing IPF Clinical Evaluation: History, PE, CXR, PFTs, 6MWT Not IIP Potential IIP HRCT Diagnostic of IPF or other diffuse lung disease Diagnosis uncertain Transbronchial Bx or BAL Diagnostic Nondiagnostic Surgical lung biopsy Not IPF IPF Adapted from ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2002;165:277-304.