Download
1 / 54
550 likes | 775 Views
MECCANISMO DI PLACENTAZIONE NORMALE.

E N D
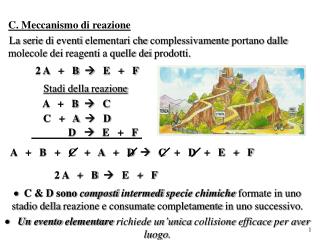
MECCANISMO DI PLACENTAZIONE NORMALE • Lo stadio più precoce del rimodellamento vascolare (FASE 1) è rappresentato dalla vacuolizzazione endoteliale e dal rigonfiamento di alcune cellule muscolari della tunica media. Tale fase rappresenta il rimodellamento vascolare indipendente dal trofoblasto ed invece correlato alla decidualizzazione. • Nella fase successiva (FASE 2) si verifica una disorganizzazione della tunica media con ampliamento degli spazi intercellulari determinando un’alterazione e perdita della tunica muscolare. Le modificazioni in questo stadio sono dipendenti dall’invasione del trofoblasto nel tessuto stromale e perivascolare, il quale determina cambiamenti nella matrice extracellulare tramite la secrezione di specifici enzimi. • La FASE 3 è caratterizzata dalla comparsa del trofoblasto endovascolare all’interno del lume vasale.
MECCANISMO DI PLACENTAZIONE NORMALE 2 • In un secondo tempo il trofoblasto endovascolare viene incorporato nella parete vasale, processo che risulta essere accompagnato dalla deposizione di materiale fibrinoide (FASE 4). L’originale strato muscolare liscio e la tunica elastica sono sostituiti da tale materiale fibrinoso, mentre le cellule trofoblastiche intercalate conferiscono, per la loro distribuzione scarsamente organizzata, un aspetto a ragnatela. • L’ultimo stadio (FASE 5) è caratterizzato dalla riparazione endoteliale a volte associata all’ispessimento intimale legato alla proliferazione delle cellule miointimali di origine materna (Pijnenborg 2006). • l’assenza delle modificazioni fisiologiche, legate ad una alterata invasione trofoblastica o al fallimento della stessa, sembrerebbe essere associata allo sviluppo della preeclampsia
Circolazione uterina (Bonnar et al: Pregnancy induced hypertension, 1980) Arterie spirali Utero non gravido sezione a livello della giunzione endometrio/miometrio Arterie spirali Secondo trimestre
Invasione endometrio e terzo interno miometrio Invasione limitata all’endometrio RIDUZIONE DELLA PORTATA EMATICA UTERO-PLACENTARE Invasione trofoblastica delle arterie utero-placentari GRAVIDANZE NORMALI PRE-ECLAMPSIA - IUGR Art. spirale
Imbalance of angiogenic factors sFlt1 VEGF, PIGF PREECLAMPSIA PREECLAMPSIA Placentation and Preeclampsia: current hypotesis Disfunctional maternal endothelium
I punti deboli della teoria corrente • La mancata invasione trofoblastica si ha solo dopo la 12^ settimana (Jauniaux, Am J Pathol 2000,157:2111) • Nel 1^ trimestre sono già presenti nel sangue delle madre i markers sierici della PE
NUOVI MODELLI PATOGENETICI • Le ipotesi attuali associano lo sviluppo della patologia a diverse alterazioni così riassunte: • effetti deleteri a livello del trofoblasto extracellulare; • fallimento dell’invasione trofoblastica nelle arterie spirali; • riduzione del flusso di sangue materno nello spazio intervilloso; • ipossia alternata ad episodi di riossigenazione della placenta; • danno ipossico al trofoblasto villoso; • rilascio di frammenti di membrana del sinciziotrofoblasto (STBM, SyncytioTrophoBlast Membrane fragments) nella circolazione materna; • risposta infiammatoria materna in seguito alla presenza degli STBM (Huppertz 2008a).
Progenitrici dello stroma placentare Progenitrici dell’embrione Progenitrici del trofoblasto Prime fasi dello sviluppo embrionale Massa cellulare interna Morula Blastocisti
Lo sviluppo precoce del trofoblastoHuppertz Hypertension 2008,51:970
Morula Prima differenziazione verso la linea trofoblastica fallimento PE & FGR Blastocisti Differenziazione in citotrofoblasto e sinciziotrofoblasto fallimento PE & FGR Precoce citotrofoblasto e sinciziotrofoblasto Differenziazione verso Trofoblasto villoso Differenziazione verso Trofoblasto extravilloso fallimento fallimento PE FGR Citotrofoblasto villoso e sinciziotrofoblasto villoso Citotrofoblasto extravilloso Figura 3.1
Due vie differenti alla PE e all’IUGRHuppertz Hypertension 2008,51:970
Towards trophoblast lineage • Abortion • PE+IUGR Failure Towards cytotrophoblast and syncytiotrophoblast Towards villous trophoblast Towards extravillous trophoblast Failure Failure PREECLAMPSIA IUGR Trophoblast lineage and PE\IUGR origin Huppertz Hypertension 2008,51:970, mod
LATE ONSET Normally grown baby Normal uterine spiral arteries Normal umbelical arteries blood flow Enlarged placental mass EARLY ONSET Inadequate trophoblast invasion Abnormal uterine arteries blod flow Abnormal umbelical arteries blood flow Intrauterine growth restriction (IUGR) Due forme di Pre-eclampsia
Burton, 2009 Placental debris Il passaggio di materiale trofoblastico nel sangue maternoHuppertz e Kingdom J Soc Gynecol Investig 2004,11:353
Stress or necrosis in maternal-fetal surface Increased expression of Damage Associated Molecular Pattern (DAMPs) (DNA, heat shock proteins, uric acid, etc) Activation of dendritic cells The danger model suggests that, if preeclampsia is an immune disease, the initial factor is not the fetal antigen recognition, but rather recognition of DAMPs generated by poor placentation
EXTRINSIC\MATERNAL FACTORS EXTRINSIC\MATERNAL FACTORS INTRINSIC PLACENTAL FACTORS Increased Placental Mass Surface increased adequate inadequate Inadequate Maternal Response or Removal Aponecrosis Apoptosis Overload of Apoptotic Removal Syncytial Knots Non-apoptotic Trophoblast Fragments Engulfment of Apoptotic Particles in the Lung Secondary Necrosis of Apoptotic Particles Sistemic Effects of Necrotic Material PREECLAMPSIA PREECLAMPSIA NORMAL PREGNANCY L’ipotesi sulla origine placentare della PE Huppertz Hypertension 2008,51:970, mod Villous Trophoblast Differentiation Villous Trophoblast Differentiation
Fattori intrinseci placentari Citotrofoblasto Villoso differenziazione adeguata inadeguata Aumento della massa/superficie Placentare: -diabete -gravidanza multipla -ipossia (anemia, elevate altitudini) Sinciziotrofoblasto Villoso Fattori estrinseci differenziazione adeguata inadeguata Apoptosi Aponecrosi/Necrosi aumentano Syncytial Knots STBM Fattori materni Inadeguata risposta o rimozione materna Sovraccarico della rimozione apoptotica Eliminazione delle particelle apoptotiche a livello polmonare Effetti sistemici del materiale necrotico Secondaria necrosi delle particelle apoptotiche PREECLAMPSIA Gravidanza fisiologica PREECLAMPSIA Figura 3.2
HANDBUCH DER GEBURTSHILFEDoderlin A. (Editor), Wiesbaden,1916 Eklampsie ZWEIFEL P. “Eclampsia is a disease of theories” OGGI: fallimento della differenziazione del trofoblasto villoso con successivo rilascio esagerato di materiale trofoblastico all’interno della circolazione materna. STBM responsabili di una risposta infiammatoria materna esagerata con conseguente esordio della preeclampsia
Nella patologia preeclamptica il rilascio del materiale proveniente dal sinciziotrofoblasto non segue le normali regole, infatti, a causa di una alterazione precoce nel processo di differenziazione del trofoblasto villoso, il rilascio dei “syncytial knots” non rappresenta più il principale meccanismo di eliminazione a disposizione, ma predominano altri processi come la necrosi e l’aponecrosi (Formigli 2000). • L’aumento dei frammenti necrotici del trofoblasto si riscontra esclusivamente nella preeclampsia, mentre nelle gravidanze complicate da FGR i livelli sono normali (Goswami 2006). • I frammenti trofoblastici necrotici rilasciati, chiamati STBM, hanno dimensioni tali (200-600 nm) (Gupta 2005) da poter oltrepassare il filtro polmonare indenni, in modo tale da persistere nel sangue periferico materno, determinando alterazioni sistemiche a carico dell’endotelio materno e del processo infiammatorio.
THE RELATION BETWEEN TROPHOBLAST DEVELOPMENT AND MARKER APPEARANCE • Biochemical markers of preeclampsia are circulating factors, whose measurement could potentially aid its diagnosis or prediction • Some are products of trophoblast or of the adjacent decidua and reflect the placental dysfunction which is an important aspect of the pathogenesis of pre-eclampsia • Others reflect the systemic responses of maternal systems to abnormal pregnancy that may be inflammatory or metabolic.
Mesenchymal Villi (4 to 23 weeks) Villous growth Immature Intermediate Villi (8 to 23 weeks) Trophoblast and Villous Development Pregnancy Implantation Delivery Maternal blood flow through the placenta Stem Villi (17/20 to 40 weeks) Villous stabilization Mature Intermediate Villi (25 to 40 weeks) Nutritional exchange Terminal Villi (27 to 40 weeks) from 34 w the dominating type of villi By courtesy of P. Kaufmann
Angiogenic Factors PlGF (VEGF) sFlt-1 sEndoglin where do they come from?
Trophoblast Development and Marker Appearance • Villous Trophoblast • Cytotrophoblast • PlGF • Flt-1 • Endoglin • Syncytiotrophoblast • PlGF • sFlt-1 • sEndoglin • Extravillous Trophoblast • PlGF • sFlt-1 • sEndoglin (?) Maternal Tissues • PlGF • sFlt-1 • sEndoglin • VEGF
What about marker appearance in maternal blood?
sFlt-1 in maternal blood Changes in circulating level of angiogenic factors from the first to second trimester as predictors of preeclampsia. Vatten LJ, Eskild A, Nilsen TI, Jeansson S, Jenum PA, Staff AC Am J Obstet Gynecol. 2007 Mar;196(3):239.e1-6.
PlGF in maternal blood Changes in circulating level of angiogenic factors from the first to second trimester as predictors of preeclampsia. Vatten LJ, Eskild A, Nilsen TI, Jeansson S, Jenum PA, Staff AC Am J Obstet Gynecol. 2007 Mar;196(3):239.e1-6.
PP13 in the placenta Galectin, highly expressed in syncitiotrophoblast. Involved in placental implantation and maternal artery remodelling
Trophoblast Development and Marker Appearance • Villous Trophoblast • Cytotrophoblast • PlGF • Flt-1 • Endoglin • Syncytiotrophoblast • PlGF • sFlt-1 • sEndoglin • PP13 • Extravillous Trophoblast • PlGF • sFlt-1 • sEndoglin (?) Maternal Tissues • PlGF • sFlt-1 • sEndoglin • VEGF
PP13 in maternal blood Longitudinal determination of serum placental protein 13 during development of preeclampsia. Huppertz B, Sammar M, Chefetz I, Neumaier-Wagner P, Bartz C, Meiri H. Fetal Diagn Ther 24:230-6 (2008) 5.1 – 56.6 weeks after LMP maternal serum Nutritional exchange Weakness: Only 4 late-PE cases -> 51 blood samples with 41 normal cases -> 440 blood samples and 18 unaffected cases -> 169 blood samples
Cell-free fetal DNA (fetal): elevated levels starting at 17 weeks ADAM12 (maternal/fetal; low in trisomies 18 and 21): decreased levels in the first trimester, interfers with adhesion and implantation PAPP-A (maternal/fetal?): widely used in trisomy screening, a protease for IGFBP-4, decreased levels cause decreased levels of free IGF. Decreased levels in the first trimester? only 8-23% of PE cases can be detected, not specific for PE (IUGR) Other Placental Markers for Preeclampsia in Maternal Blood
Trophoblast Development and Marker Appearance • Villous Trophoblast • Cytotrophoblast • PlGF • Flt-1 • Endoglin • fetal DNA/RNA • ADAM12 • PAPP-A • Syncytiotrophoblast • PlGF • sFlt-1 • sEndoglin • PP13 • fetal DNA/RNA • ADAM12 • PAPP-A • Extravillous Trophoblast • PlGF • sFlt-1 • sEndoglin (?) • fetal DNA/RNA • ADAM12 (?) • PAPP-A (?) Maternal Tissues • PlGF • sFlt-1 • sEndoglin • VEGF
Trophoblast Development and Marker Appearance • Villous Trophoblast • Cytotrophoblast • PlGF • Flt-1 • Endoglin • fetal DNA/RNA • ADAM12 • PAPP-A • Syncytiotrophoblast • PlGF • sFlt-1 • sEndoglin • PP13 • fetal DNA/RNA • ADAM12 • PAPP-A • Extravillous Trophoblast • PlGF • sFlt-1 • sEndoglin (?) • fetal DNA/RNA • ADAM12 (?) • PAPP-A (?) • Maternal Tissues • P-selectin • Pentraxin-3 • PlGF • sFlt-1 • sEndoglin • VEGF
PTX3: belongs to famiy of pentraxins, involved in inflammation, like CRP A multifunctional soluble Pattern Recognition Receptor (Garlanda C., Ann. Rev. Immunol. 2005)
CELLULAR SOURCES OF PTX3 (Garlanda C., Ann. Rev. Immunol. 2005)
PTX3 as a novel diagnostic tool: a working hypothesis A new marker for inflammatory disorders reflecting in particular the involvement of the vascular bed. (Peri G, Circulation 2000) (Klouche M, Atherosclerosis 2004)
Pre-existing maternal endothelial dysfunction. Metabolic syndrome Obesity Insulin resistance Hyperglycemia Hyperlipidemia Excessive proinflammatory status (cytokines) Placental insufficiency IUGR PREECLAMPSIA
PTX3 levels throughout the three trimesters in normal pregnancies compared to non-pregnant women. PTX3 levels increase in pregnancy, but do not change significantly throughout the three trimesters of normal pregnancies. PTX3 single values with respective median levels. p<0.001 Cetin I. et al. Am.J.Obstet.Gynecol. 2006
PTX3 maternal levels in preeclampsia and IUGR vs normal pregnancies. *** PTX3 levels in preeclampsia are significantly higher compared to normal pregnancies of corresponding gestational age. IUGR showed intermediate levels. ** * n=26 n=16 n=20 Maternal plasma median levels and interquartile range. ***p<0.001; **p<0.01;*p<0.05 Cetin I. et al. Am.J.Obstet.Gynecol. 2006
Patrizia Rovere-Querini et al.Plasma and Tissue Expression of the Long Pentraxin 3 During Normal Pregnancy and PreeclampsiaObstet Gynecol 2006;108:148–55) Fig. 2 - Higher circulating levels of PTX3 in patients with preeclampsia.
PTX3 maternal levels in relation to severity of preeclampsia The severity of the disease is associated to maternal PTX3 levels. *** ** *** n=32 n=15 n=30 Maternal plasma median levels. °°°p<0.001; **p<0.01 Cetin I. et al. manuscript in preparation
Placenta: stroma of stem villi and anchoring villi Normal Preeclampsia NO DIFFERENCES for immunostaining (brown) for PTX3 localization in the stroma of the stem villi (panel a-c) and in the anchoring villi (panels b-d) in normal (a-b) and preeclamptic (c-d) placentas.
Maternal peritoneum PTX3 localization in the parietal peritoneum in a case of IUGR. Strong endothelial signal in the peritoneum of a preeclamptic case.
HYPOTHESIS PTX3: New marker of altered endothelial function, typical of preeclampsia. • Causal or consequential role in pregnancy complications? • Early biomarker for the prediction of adverse pregnancy outcome?
I Cetin, V Cozzi, AT Papageorghiou, V Maina, A Montanelli, C Garlanda, B ThilaganathanFirst trimester PTX3 levels in women who subsequently develop preeclampsia and fetal growth restrictionActa Obstetricia et Gynecologica Scandinavica,2009; 88:7,846 — 849 Prospective maternal plasma collection from pregnant women at 11-14 week of gestation. Outcome: preeclampsia, IUGR Table I - Maternal demographic characteristics and pregnancy outcomes in the study groups.
I Cetin, V Cozzi, AT Papageorghiou, V Maina, A Montanelli, C Garlanda, B ThilaganathanFirst trimester PTX3 levels in women who subsequently develop preeclampsia and fetal growth restrictionActa Obstetricia et Gynecologica Scandinavica,88:7,846 — 849 PTX3 levels are elevated in women who subsequently develop preeclampsia, but are normal in those with IUGR. PTX3 levels as mean (diamonds) ± SD (box) and respective range (whiskers). *** p<0.001.
I Cetin, V Cozzi, AT Papageorghiou, V Maina, A Montanelli, C Garlanda, B ThilaganathanFirst trimester PTX3 levels in women who subsequently develop preeclampsia and fetal growth restrictionActa Obstetricia et Gynecologica Scandinavica,88:7,846 — 849 The median CRP levels did not vary significantly between the three groups (p=0.26)
R Akolekar, D Casagrandi, P Livanos, A Tetteh and K H NicolaidesMaternal plasma pentraxin 3 at 11 to 13 weeks of gestation in hypertensive disorders of pregnancyPrenat Diagn (2009) Table 2—Median (interquartile range) for plasma pentraxin 3 and uterine artery pulsatility index (PI) in the outcome groups