Download
1 / 45
690 likes | 2.53k Views
DIFFICULT AIRWAY MANAGEMENT. PP CHEN Department of Anaesthesia & Operating Services Alice Ho Miu Ling Nethersole Hospital. What is a difficult airway?. Difficult manual ventilation Difficult tracheal intubation. Adverse effects of difficult airway. Hypoxia Cardiac arrest Encephalopathy

E N D
DIFFICULT AIRWAY MANAGEMENT PP CHEN Department of Anaesthesia & Operating Services Alice Ho Miu Ling Nethersole Hospital
What is a difficult airway? • Difficult manual ventilation • Difficult tracheal intubation
Adverse effects of difficult airway • Hypoxia • Cardiac arrest • Encephalopathy • Other organs involvement • Aspiration pneumonitis
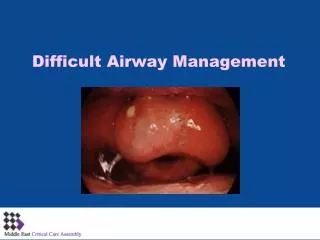
Predicting difficult airway & tracheal intubation • Limited neck (C-spine) movement • Receding chin (mandible) • Prominent maxilla • Short, muscular, obese neck • Limited mouth opening • Bucked teeth, missing teeth with gaps • Large tongue • High arch palate • High anterior larynx
Mallampati Grading • Samsoon & Young modification • Grade 1 Faucial pillar & uvula, soft palate all seen • Grade 2 Faucial pillar & uvula masked by base of tongue • Grade 3 Soft palate, base of uvula seen • Grade 4 Even soft palate not seen
TM Distance > 6.5cm = easy 6-6.5cm = difficult <6cm = impossible
Wilson risk score • Weight • Head & neck movement • Jaw movement • Receding mandible • Bucked teeth • Risk score 0,1,2 for each category
Predicting difficult airway & tracheal intubation • Morbid obesity, pregnancy • Ankylosing spondylitis • Trauma eg C-spine, facial injuries • Burns to face & neck with contractures • Postradiotherapy • Congenital eg Pierre Robin syndrome • Inhalational burn injury • Infection eg epiglotitis, dental, quinsy • Neoplasm • Endocrine eg thyroid enlargement
Managing manual ventilation • Triple manouevre • Head tilt • Chin lift • Jaw thrust
Preparation for Tracheal intubation 1 • Prepare and check • intubation equipment • Laryngoscopes, ETTs (3 sizes), guides (stylet, bougie), syringe, tie or sticky tape, scissor, lubricant • suction device • Yankauer sucker, suction catheter, suction pressure • oxygen supply & ventilation equipment • manual resuscitator, facemasks, airways
Preparation for tracheal intubation 2 • Establish iv access • Preoxygenate patient • Prepare drugs for anaesthesia • Choices • Thiopentone, Propofol, Etomidate, Midazolam, Ketamine • Suxamethonium, Cisatracurium, Atracurium, Rocuronium, Vecuronium, Pancuronium • Fentanyl, other opioids
Positioning for tracheal intubation • Sniffing position • Flexion of cervical spine • Extension of atlanto-occipital joint
Awake Fibreoptic intubation Using Local anaesthetic to intubate tracheal via mouth or nose before induction of anaesthesia
Berman Airway Ovassapian Airway
Other laryngoscopes • Bullard laryngoscope • Upsher scope • WuScope
Mx of difficult intubation 1 • Inability to open mouth • Give more relaxant or wait longer for it to work if inadequate relaxation • Perform intubation under LA + sedation if mechanical obstruction to mouth opening • Dental gaps (as the result of removed denture) may make it difficult to visualise vocal cords • Use gauze roll to fill gaps • Short, fat neck, large breast in the obese or pregnant patient • Awake fibreoptic intubation • Polio blade
Mx of difficult intubation 2 • Vocal cord partially visible • Make sure head & neck are in optimal (sniffing) position • Push on front of neck to make larynx more posterior • Use stylet, gum elastic bougie • Vocal cord not visible but epiglottis visible • Use gum elastic bougie • Consider fibreoptic intubation if difficult with bougie • Epiglottis not visible • Use long laryngoscope blade • Fibreoptic intubation
Failure to Intubate Call for HELP Mask Ventilation Adequate? YES NO Intubation Choices LMA TTJV Combitube FAIL SUCCEED SUCCEED FAIL Surgical Airway Surgical Airway Intubation Choices CONFIRM Difficult Airway Algorithm