Download
1 / 24
270 likes | 756 Views
DENGUE FEVER. IRAM FATIMA. Dengue Fever. Dengue virus Most prevalent vector-borne viral illness in the world Main mosquito vector is Aedes aegypti Year round transmission. Incidence. 50-100 million dengue fever infections per year globally

E N D
DENGUE FEVER IRAM FATIMA
Dengue Fever • Dengue virus • Most prevalent vector-borne viral illness in the world • Main mosquito vector is Aedes aegypti • Year round transmission
Incidence • 50-100 million dengue fever infections per year globally • 500,000 cases of severe dengue, dengue hemorrhagic fever or dengue shock syndrome • 100-200 cases annually in U.S. • Average case fatality 5% • IN 2011 in pakistan 12000 cases and 165 deaths,,cases reported
Distribution • Endemic in more than 100 tropical and subtropical countries • Pandemic began in Southeast Asia after WW II with subsequent global spread • Several epidemics since 1980s • Distribution is comparable to malaria
Virology • Flavivirus family • Small enveloped viruses containing single stranded positive RNA • Four distinct viral serotypes (Den-1, Den-2, Den-3, Den-4)
Pathophysiology • Transmitted by the bite of Aedes mosquito (Aedes aegypti) • Incubation 3-14 days • Acute illness and viremia 3-7 days • Recovery or progression to leakage phase
Pathophysiology • Dengue virus enters and replicates within monocytes, mast cells, fibroblasts • Innate and adaptive immune response • Cytokine release: TNF-a, IL-2, IL-6, IL-8 • Compliment activation • T-cell activation: CD4 and CD8 cells cytokine production
Pathophysiology Capillary Leak Syndrome: • Transient increased capillary permeability due to endothelial cell dysfunction • Widening of tight junctions • Cytokine release and complement activation Leukopenia, Thrombocytopenia and Hemorrhagic diathesis: • Direct viral bone marrow suppression • Platelet destruction in DHF • ?Molecular mimicry between viral protein and coagulation factors
Clinical Presentation • Spectrum of illness • non-specific febrile illness • classic dengue • dengue hemorrhagic fever • dengue shock syndrome • other (CNS dysfunction, liver failure, myocarditis)
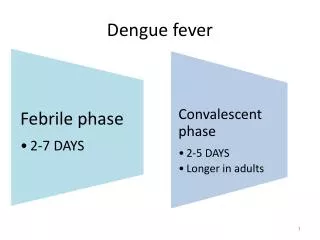
Classic Dengue • Acute febrile illness with headache, retro-orbital pain, myalgias, arthralgias • “Break-bone fever” • High fever 5-7 days • Second fever for 1-2 days in 5% patients • Followed by marked fatigue days to weeks • Classic dengue 15-60% of infections • Nausea, vomiting, diarrhea (30%) • Macular or maculopapular confluent rash (50%) • Respiratory symptoms: cough, sore throat (30%)
Dengue Hemorrhagic Fever • Usually occurs in secondary infections after actively or passively (maternal) acquired immunity to a different viral serotype • Only 2-4% of secondary infections result in severe disease • Mortality is 10-20% if untreated, but decreases to <1% if adequately treated • Plasma leakage may progress to dengue shock syndrome
Dengue Hemorrhagic Fever WHO classification of DHF • Thrombocytopenia (platelet count <100,000) • Fever 2-7 days • Hemorrhagic manifestations with a positive tourniquet test, petechiae, ecchymoses or mucosal bleeding. • Hemoconcentration or evidence of plasma leakage (ascites, effusion, decreased albumin)
Physical Exam • Nonspecific findings • Conjunctival infection, pharyngeal erythema, lymphadenopathy, hepatomegaly (20-50%) • Macular or maculopapular rash (50%)
Laboratory Findings • Leukopenia • Thrombocytopenia (<100,000) • Modest liver enzyme elevation (2-5x nml) • Serology: • Acute phase serum IgM (+6-90 days) ELISA • Acute and convalescent IgG (99% sens, 96% spec) • Hemagglutination inhibition assay (HI) is gold assay, positive if >4
Disease Factors • Dengue-2 serotype most virulent • Increased severity with secondary infections • Increased risk in children <15 years and elderly. • Greatest risk of DHF in infants. • More severe in females • Increased mortality with comorbid conditions • Less common in malnourished children
Differential Diagnosis Viral: Influenza, HIV, Hepatitis A, Yellow Fever, Hantavirus, Measles, Rubella, Coxsackie and other enteroviruses, parvovirus B19, Chikungunya virus, EBV Bacterial: Typhoid, Scarlet fever, Meningococcemia Parasitic:Malaria, Leptospirosis, Rickettsial disease, Leishmaniasis, Chagas disease Fungal: Cryptococcus, Blastomycosis, Histoplasmosis Non-Infectious: Malignancy, rheumatic, vasculitis, drug fever, other miscellaneous
Treatment • No specific therapy • Supportive measures: adequate hydration acetaminophen (if no liver dysfunction) avoid ASA and NSAIDs • DHF or DHF w/ shock: IV fluid resuscitation and hospitalization blood or platelet transfusion as needed
Treatment • Treatment with corticosteroids shown not to reduce mortality with severe dengue shock • Ribavirin very weak in vitro and in vivo activity against flaviviruses
Vaccination • No current dengue vaccine • Estimated availability in 5-10 years • Vaccine development is problematic as the vaccine must provide immunity to all 4 serotypes • Lack of dengue animal model • Live attenuated tetravalent vaccines under phase 2 trials • New approaches include infectious clone DNA and naked DNA vaccines
Prevention Biological: • Target larval stage of Aedes in large water storage containers Chemical: • Insecticide treatment of water containers • Space spraying (thermal fogs)
Prevention • Personal: • clothing to reduce exposed skin • insect repellent especially in early morning, late afternoon. Bed netting is of little utility. • Environmental: • reduced vector breeding sites • solid waste management • public education