Download
1 / 56
630 likes | 952 Views
Insulin resistance and -cell dysfunction are fundamental to type 2 diabetes. Uncontrolled hyperglycemia. Obesity. IFG. Diabetes. 350 –. Post-prandial glucose. 300 –. 250 –. Glucose (mg/dl). Fasting glucose. 200 –. 150 –. 100 –. 50 –. 250 –. Insulin resistance. 200 –.

E N D
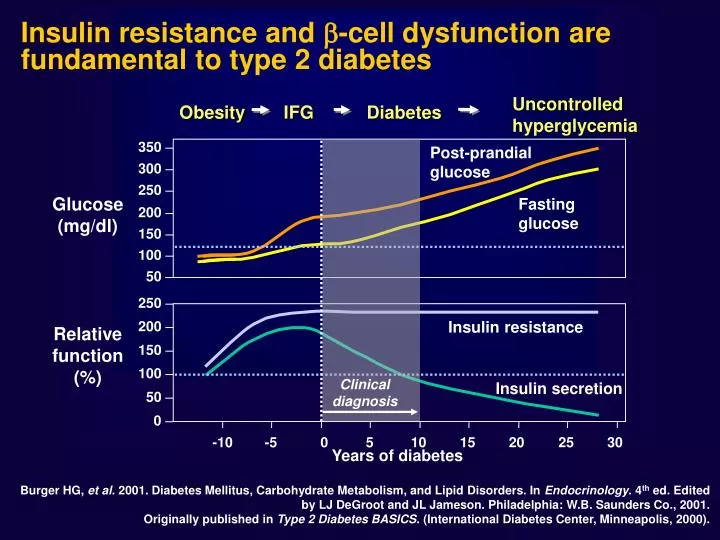
Insulin resistance and -cell dysfunction are fundamental to type 2 diabetes Uncontrolledhyperglycemia Obesity IFG Diabetes 350 – Post-prandialglucose 300 – 250 – Glucose (mg/dl) Fasting glucose 200 – 150 – 100 – 50 – 250 – Insulin resistance 200 – Relativefunction(%) 150 – 100 – Clinical diagnosis Insulin secretion 50 – 0 – -10 -5 0 5 10 15 20 25 30 Years of diabetes Burger HG, et al. 2001. Diabetes Mellitus, Carbohydrate Metabolism, and Lipid Disorders. In Endocrinology. 4th ed. Edited by LJ DeGroot and JL Jameson. Philadelphia: W.B. Saunders Co., 2001. Originally published in Type 2 Diabetes BASICS. (International Diabetes Center, Minneapolis, 2000).
Type 1 Insulin analogs Human insulin Pump therapy Insulin therapy 1900 1950 2000 1920 Type 2 Meglitinides Glitazones First human treated Alpha-glucosidase Inhibitors NPH insulin Biguanide Sulfonylureas Insulin therapy Diet 1900 1950 2000 1920 A Century of Diabetes Care
UKPDS: reduced micro- and macrovascular complications for a 1% decrease in HbA1c Any diabetes-related endpoint Diabetes- related death All cause mortality Peripheral vascular disease* Myocardial infarction Microvascular disease Cataract extraction Stroke 0 –5 21% 21% 14% 14% 12% 43% 37% 19% –10 P = 0.035 –15 P < 0.0001 P < 0.0001 –20 P < 0.0001 Percentage reduction in relative risk corresponding to a 1% fall in HbA1c P < 0.0001 P < 0.0001 –25 –30 –35 –40 P < 0.0001 –45 P < 0.0001 –50 Adapted from Stratton IM, et al. UKPDS 35. BMJ 2000; 321:405–412. *Lower extremity amputation or fatal peripheral vascular disease
EPIC-Norfolk study: Risk of CV events or Death Associated with HbA1c Level 5–5.4% HbA1c level: 5.5–5.9% 6.0–6.4% 6.5–6.9% 7% Men Women 8 7 6 5 Age-adjusted relativerisk 4 3 2 1 0 CHD events CVD events All-cause mortality CHD events CVD events All-cause mortality P 0.001 for linear trend across HbA1c categories for all endpoints. • Khaw et al. Ann Intern Med 2004; 141: 413–20
SECRETAGOGHI • Sulfoniluree: Glibenclamide Gliclazide Glimepiride • Glinidi: Repaglinide Nateglinide
ATP ADP Precondizionamento ischemico Normale K+ K+ Cellula muscolare cardiaca o coronarica Ca++ Ca++
ATP ADP Contrattilità Consumo energia Rilascio muscolo Vasodilatazione Precondizionamento ischemico Ischemia K+ K+ Cellula muscolare cardiaca o coronarica Ca++ Ca++
ATP ADP Contrattilità Consumo energia Rilascio muscolo Vasodilatazione Precondizionamento ischemico FARMACO SUR2 Ischemia K+ K+ Cellula muscolare cardiaca o coronarica Ca++ Ca++
Sulfaniluree e Preconditioning • 1: Lee TM, Chou TF. Impairment of myocardial protection in type 2 diabetic patients. J Clin Endocrinol Metab. 2003 Feb;88(2):531-7. • 2: Riddle MC. Editorial: sulfonylureas differ in effects on ischemic preconditioning--is it time to retire glyburide? J Clin Endocrinol Metab. 2003 Feb;88(2):528-30. • 3: Scognamiglio R, Avogaro A, Vigili de Kreutzenberg S, Negut C, Palisi M, Bagolin E, Tiengo A. Effects of treatment with sulfonylurea drugs or insulin on ischemia-induced myocardial dysfunction in type 2 diabetes. Diabetes. 2002 Mar;51(3):808-12. • 4: Lee TM, Su SF, Chou TF, Lee YT, Tsai CH. Loss of preconditioning by attenuated activation of myocardial ATP-sensitive potassium channels in elderly patients undergoing coronary angioplasty. Circulation. 2002 Jan 22;105(3):334-40. • 5: Ghosh S, Standen NB, Galinianes M. Failure to precondition pathological human myocardium. J Am Coll Cardiol. 2001 Mar 1;37(3):711-8. • 6: Ovunc K. Effects of glibenclamide, a K(ATP) channel blocker, on warm-up phenomenon in type II diabetic patients with chronic stable angina pectoris.Clin Cardiol. 2000 Jul;23:535-9. • 7: Tomai F, Danesi A, Ghini AS, Crea F, Perino M, Gaspardone A, Ruggeri G, Chiariello L, Gioffre PA. Effects of K(ATP) channel blockade by glibenclamide on the warm-up phenomenon. Eur Heart J. 1999 Feb;20(3):196-202.
Insulin Glibenclam. 468 4511 437 3712 p= NS p<0.05 B B D D B D
Impairment of Myocardial Protection in Type 2 Diabetic Patients: ST segment shift (mV)
BIGUANIDI • Metformina • (Fenformina)
Glucose 5 mM a Glucose 20 mM b Glucose 20 mM+ Metformin c
EFFECT OF METFORMIN IN OVERWEIGHT PATIENTS UKPDS 34. Lancet 1998;352:854-865.
Risk of Fatal and Nonfatal Lactic Acidosis With Metformin Use in Type 2 Diabetes Mellitus: Systematic Review and Meta-analysis Salpeter SR, Greyber E, Pasternak GA, Salpeter EE There is no evidence to date that metformin therapy is associated with an increased risk of lactic acidosis or with increased levels of lactate compared with other antihyperglycemic treatments if the drugs are prescribed under study conditions, taking into account contraindications. Arch Intern Med 2003;163(21):2594-602
CONTROINDICAZIONI E LINEE-GUIDA PER LA SOSPENSIONE DELLA METFORMINA BMJ, 326, 2003 • Sospendere se la creatininemia è >150 mol/l* • Sospendere durante i periodi di sospetta ipossia tissutale (per es. durante infarto del miocardio, sepsi, etc.) • Sospendere per 3 giorni dopo somministrazione di mezzo di contrasto contenente iodio e ripristinare solo dopo controllo dei parametri di funzionalità renale • Sospendere 2 giorni prima di un’anestesia generale e ripristinare quando la funzionalità renale è stabile *Qualsiasi concentrazione di creatinina venga scelta come livello cut-off per insuficienza renale sarà arbitrario in considerazione della massa muscolare dell’individuo e del turnover proteico; precauzione nel paziente anziano.
Metformina ed Acidosi Lattica Condizioni associate (% pazienti) 23 casi riportati in letteratura fino al 1978 Phillips, BMJ 1:239, 1978
Conclusions. Metformin was the only antidiabetic agent not associated with harm in patients with heart failure and diabetes. It was associated with reduced all cause mortality in two of the three studies.
Nathan DM, Buse JB, Davidson MB, et al. Management of hyperglycaemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement from the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2006;49:1711-21.
TIAZOLIDINEDIONI (GLITAZONI) • Pioglitazone • Rosiglitazone
GLUT 4 Storage granule Insulin GLUT 4 Translation Glucose Thiazolidinedione GLUT 4 RNA PPAR Transcription DNA Cytoplasm Nucleus Thiazolidinediones: mechanism of action Thiazolidinedione (rosiglitazone, pioglitazone) Adipocyte +
GLITAZONI - EFFETTI INDESIDERATI Edema Anemia (da diluizione) Ipercolesterolemia Incremento ponderale Epatopatia Insufficienza Cardiaca ALTRI: trombocitopenia, ipoglicemia, sonnolenza, vertigini, cefalea, parestesie, dolori addome, flatulenza, nausea, alopecia, rash, astenia
Prima di iniziare la terapia verificare la presenza di cardiopatia, edema, dispnea ADA-AHA 2006
STOP-NIDDM trial Effect of acarbose and placebo on cumulative probability of remaning free of diabetes over time Lancet, 2002
Le insuline nella storia Insulina porcina: non piu’ in commercio differiva da quella umana per un aminoacido Insulina bovina: non piu’ in commercio differiva da quella umana per tre aminoacidi Insulina umana: disponibile, in produzione dagli anni ‘80 non differisce da quella umana e viene prodotta con la tecnica del DNA ricombinante: piu’ pura Insulina analogo: disponibile, in produzione dal ‘96 differisce dall’umana: miglior farmacocinetica
Comparison of Human Insulins / Analogues Duration of action Insulin Onset of action Peak Regular 30–60 min 2–4 h 6–10 h NPH/Lente 1–2 h 4–8 h 10–20 h Ultralente 2–4 h Unpredictable 16–20 h Lispro/aspart 5–15 min 1–2 h 4–6 h Glargine 1–2 h Flat ~24 h
Basal/Bolus Treatment Program withRapid-acting and Long-acting Analogs Breakfast Lunch Dinner Aspart Aspart Aspart or or or Lispro Lispro Lispro Plasma insulin Glargine or Detemir 4:00 8:00 12:00 16:00 20:00 24:00 4:00 8:00 Time
Scopi del trattamento insulinico intensivo • Mantenere la normoglicemia • Evitare le complicanze acute • Evitare o arrestare la progressione delle complicanze croniche • Migliorare la qualità di vita
GLP-1 • “Incretin” hormone secreted by jejunal and ileal L cells in response to a meal • Stimulates insulin secretion • Decreases glucagon secretion • Slows gastric emptying • Reduces fuel intake (increases satiety) • Improves insulin sensitivity • Increases b-cell mass and improves b-cell function (animal studies)
Cellule K – tratto GI prossimale (duodeno e digiuno prossimale) ProGIP GIP (1-42) Cellule L – tratto GI distale (ileo e colon) Proglucagone GLP 1(7-37) GLP 1(7-36)NH2 GIP = polipeptide insulinotropico glucosio-dipendente GLP 1 = peptide 1 glucagone-simile • Stimola la secrezione di insulina in maniera glucosio-dipendente • Promuove la proliferazione e la sopravvivenza delle cellule beta in colture di isole pancreatiche Adattato da Drucker DJ DiabetesCare 2003;26:2929–2940; Ahrén B Curr Diab Rep 2003;3:365–372;Drucker DJ Gastroenterology 2002;122:531–544; Farilla L et al Endocrinology 2003;144:5149–5158; Trümper A et al Mol Endocrinol 2001;15:1559–1570; Trümper A et al J Endocrinol 2002;174:233–246.