Download
1 / 8
80 likes | 258 Views
Use of Nutrition Corners to Improve Identification and Nutritional Status of HIV-Infected Infants and Young Children in Lesotho. Presented by: Malijane Nyabela Co-authors: A. Tiam, T. Isavwa, L. Buhendwa Abstract Number: TUAD0901 December 6, 2011. Background.

E N D
Use of Nutrition Corners to Improve Identification and Nutritional Status of HIV-Infected Infants and Young Children in Lesotho Presented by: Malijane Nyabela Co-authors: A. Tiam, T. Isavwa, L. Buhendwa Abstract Number: TUAD0901 December 6, 2011
Background • Lesotho has a population of about 1.87 million and HIV prevalence of 23.7% (270,000 people including 37,000 children) • Lesotho is faced with both challenges of HIV and under-nutrition, as 2009 LDHS report shows: • 39% children under 5 years of age being stunted • 13% underweight • 4% wasted (acute malnutrition) • Evidence suggest that HIV prevalence is especially high (28.7%) among undernourished children1 • There has been an observed increase in the proportion of HIV-infected children admitted with severe malnutrition in Lesotho2 • EGPAF embarked on establishing Nutrition Corners in 17 hospitals, from 2009 to 2011, throughout Lesotho to combat risk factors that can increase severe Malnutrition in hospitals. (e.g., inadequate knowledge, skills and unsafe feeding practices by caregivers) O’Hare, 2009 Lesotho National Nutrition Survey(LNNS) report 2007
Nutrition Corner Goals and Objectives Main goals: To prevent malnutrition among children under 5 through integration of nutritional supportive counseling directed toward caregivers in four rural hospitals in Lesotho within MNCH services, and to improve growth, development and overall health of Basotho children. Objectives:
Services at the Nutrition Corner • Anthropometric measurements (weight, height and mid-upper arm circumference) • Screening for severity of under nutrition using WHO weight–for-height reference card • Referral of children to appropriate rehabilitative programs (e.g., outpatient therapeutic or feeding programs) • Demonstration of how to prepare complementary foods using locally available ingredients • Education and counseling of caregivers on basic nutrition issues and good infant and young child feeding (IYCF)practices
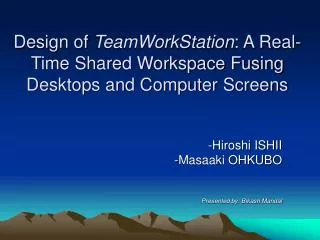
Program Assessment • Piloted in four rural hospitals (one in Butha-Buthe, one in Leribe, and two in Thaba-Tseka) by EGPAF and MOH • Conducted a review of all children under five years of age who were presenting with under nutrition and whose mothers were confirmed HIV-positive. • EGPAF collected data twice per month in all four facilities from August 2009 to February 2010 Red highlighted districts = location of pilot facilities
Results • Total of 293 children (mean age = 30 months) were enrolled in the 4 nutrition corners • 170 (58%) of 293 had unknown HIV status and were tested for HIV at the corners • 10 (5.9%) were confirmed HIV infected • 8 out of 10 (80%) HIV-infected children presented with moderate under nutrition • All 10 children were enrolled into treatment • 6 out of 10 were enrolled into ART corners • 4 out of 10 were enrolled into MNCH (DBS) corners • Of the 293 enrolled children, 165 presented with moderate under nutrition and were eligible for rehabilitation with therapeutic food in the form of Plumpy’nut. • They were seen every 2 weeks for a period of 6 months while monitored closely by the nutrition assistant or nurse to ensure they were taking the food appropriately. • At every visit they were screened for improvement in their nutritional status. • During the first 4 months, 94 (57%) children out of 165 improved significantly from moderate under nutrition to normal weight/height distribution (z-scores) with a mean z-score of 95% (< median > -1 SD)3 3 WHO weight-for-height reference card
Lessons Learned and Next Steps • Integrating HIV testing in nutrition corners is effective in linking HIV-infected children to ART services in Lesotho. • Nutrition corners will be scaled up to other hospitals and clinics in the country. • It is recommended that this approach be explored in other sub-Saharan African countries to prevent and eliminate pediatric under nutrition in HIV endemic areas.

![EVM System Surveillance Presented By: [NAMES] Presented to: [GROUP]](https://cdn0.slideserve.com/294105/slide1-dt.jpg)