Download
1 / 10
100 likes | 203 Views
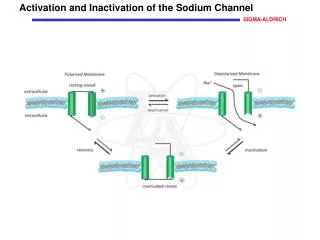
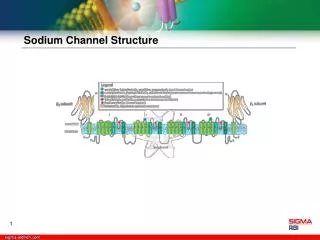
Ten Minute Toxicology- Sodium Channel Blockade. Russell Berger, MD Co-Director of Medical Toxicology Cambridge Health Alliance. Pathogenesis of Na Channel Blockade. Examples of Na Channel Blockers. TCA’s Benadryl Carbamazepine Propanalol Darvocet Chloroquine Quinine Many others….

E N D
Ten Minute Toxicology-Sodium Channel Blockade Russell Berger, MD Co-Director of Medical Toxicology Cambridge Health Alliance
Examples of Na Channel Blockers TCA’s Benadryl Carbamazepine Propanalol Darvocet Chloroquine Quinine Many others…
Recognition of Na Channel blockade • Is QRS > 100ms • Is R wave in AVR > 3mm • Is there a significant change in the patient’s QRS complex with respect to their baseline QRS (established on prior ekgs)?
Why we care… • QRS > 120 = Seizures • QRS >160 = Vtach and Vfib…death
Treatment • Na Bicarbonate: • Bolus with amps of Na bicarb until drip is available -3 amps of Na bicarb in D5W as drip LIMITATION: Serum pH
Treatment Continued When serum pH limit is reached Hypertonic Saline -4-5cc/kg boluses PRN continued seizures or ventricular dysrhtymias. LIMITATION: Serum Sodium
Treatment Continued When serum Na limit is reached Intralipid 20 % intralipid solution 1.5 cc/kg bolus 0.25cc/kg/min as a drip x1 hour Limitation: Interpretation of basic lab parameters 2/2 lipemia; pancreatitis
Finally • Consider transfer for ECMO or IABP therapy with refractory severe toxicity manifest by status epilepticus, refractory hypotension, or dysrhythmias.