Download
1 / 49
490 likes | 824 Views
Regional Biomechanics Hip Joint. Kinematics Kinetics Pathomechanics. Kinematics. Bone Structure Capsule Ligaments Muscles. 1-Bony Articulation. Femoral Head (Superiorly, Medially, Anteriorly). Acetabulum (Inferiorly, Laterally, Anteriorly). Horseshoe-shaped (Acetabular Notch).

E N D
Regional BiomechanicsHip Joint Kinematics Kinetics Pathomechanics
Kinematics • Bone Structure • Capsule • Ligaments • Muscles
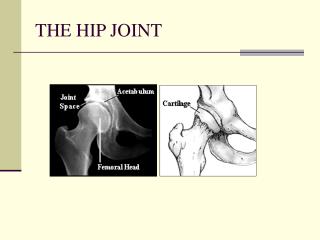
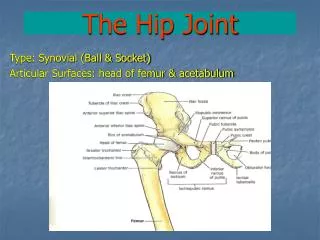
1-Bony Articulation • Femoral Head (Superiorly, Medially, Anteriorly). • Acetabulum (Inferiorly, Laterally, Anteriorly). Horseshoe-shaped (Acetabular Notch). The deepest portion (Acetabular Fossa). Labrum Acetabular: Is a wedged fibrocartilaginous ring inserted into the acetabular rim to increase the acetabular concavity.
Angles of Hip Joint(1)Center edge angle • Seen in frontal Plane. • Between two lines: 1stline: Vertical line & center of the head. 2nd line: Lateral rim & center of the head. • Average value: 22-42 degree. • Function: Provide lateral stability of the pelvis “Coverage". Prevent superior dislocation. • Increased with age: that is why congenital hip dislocation is common in children ( diminished CE angle)
(2)Angle of Inclination • Seen in frontal Plane. • Lies between anatomical axis of the neck and femoral shaft. • Average value:150 in infancy & decreased to 120 degrees in adults. Pathological increase is Coxa Valga while Pathological decrease is Coxa Vara . • Function: Allow high degree of freedom. ”by moving the longitudinal axis of the femur away from the hip joint”. - N.B:The mechanical axis is a line from the femoral head center to the midpoint of femoral condyles. It makes 5-7 degrees with the anatomical axis.
(3) Acetabular Anteversion Angle • Seen in horizontal Plane. • 1st line: Anteroposterior vertical line to the posterior rim. • 2nd line: Line connect the anterior and posterior rim. • 20 degrees. • Reason: Femoral condyles align themselves so the knee joint axis lies in the frontal plane. • Function: Prevent anterior hip joint dislocation.
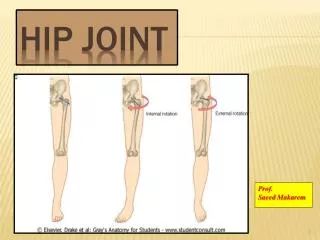
(4)Angle of Torsion • Transverse Plane. • Lies between the axis of the femoral neck and the axis of the femoral condyles “Frontal plane”. • Facing anteriorly. • 10-15 degrees. decreased with age. 40 degree in Newborn. • Reason: Femoral condyles align themselves so the knee joint axis lies in the frontal plane. • Function: 1- play a role in the hip stability. 2- one of the possible causes of excessive internal or external hip joint rotation. 3- prevent threatening of congruency during torsion.
2- Capsule of the hip joint • Strong, Dense, Shaped like a cylinder sleeve. • Attachment: Periphery of acetabulum and cover neck femoral neck. • Thick anterosuperiorly, relatively thin and loosely poster inferiorly. • Capsule has 4 sets of fibers 1- Longitudinal 2- Oblique 3- Arcuate 4- Circular
3- ligaments(1) Iliofemoral ligament • Position: Fan-shaped, inverted letter Y. The thickest and strongest ligament. In front of Jt. • Attachment: Apex ”ASIS” Base “trochanteric” line. Superior band “stronger”. Inferior band. • Orientation: Downward, Inferior, & Lateral. • Function: 1-limits hyperextension. 2-tight during Adduction. 3- Check both lat. & med. Rotation.
(2) Pubofemoral Ligament • Position: Narrow band, Lower antermedial aspect • Attachment: Superior pubic ramus to just at the end of anterior capsule. • Orientation: Downward, Inferior,& Lateral. • Function: 1- Resist abduction & Extension. 2- Tense in lat. rotation and relax in med. rotation
a) Superior band b) Inferior band B) & C) behavior of iliofemoral & pubofemoral in hip adduction and (C) adduction
(3)Ischiofemoral ligament • Position: Wide band on the posterior aspect, Triangular shape. • Attachment: post. & Inf. Aspect of acetabulum. To inner surface of greater trochanter. • Orientation: Outward & Anterior • Function: 1- Superior fibers tight during extension, add. &med. Rotation. 2- Inferior Fibers tight during flexion.
(4)Ligamentum Teres • Position: Inside the Joint, flat, narrow triangular. Three bundles: Post ischial , Ant Pubic & Intermediate bundle • Attachment: Apex at fovea capitis to acetabular notch. • Orientation: downward. • Function: Minimal mechanical role. It contributes to the vascular supply of the femoral head.
Muscles of the hip joint • Flexors: “Iliopsoas”, rectus femoris, sartorius, tensor fascia lata, pectineus, Add Longus, magnus & gracilis. • Extensors: “GL Maximus”, hamstring, GL Medius, Add magnus, Piriformis. • Adductors: Pectineus, Add. Brevis, Longus & magnus and gracilis. • Abductors: “GL Medius & Minimus” Maximus, sartorius, tensor fascia lata. • Lat Rotators: Obturator internus & externus. Gemellus Sup&Inf. Quadratus femoris & Piriformis. • Med Rotators: No ms with primary function. But Anterior portion GL medius & tensor fascia lata.
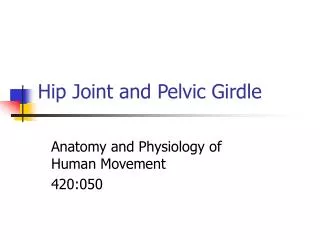
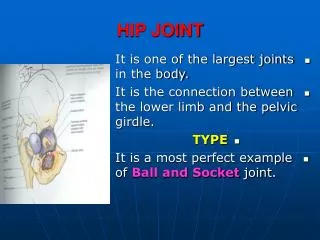
Functions of the hip joint 1- Support (HAT) 2- Closed Kinematic Chain: both the proximal and distal end is fixed. 3- Provide a pathway for the transmission of force between the pelvis and lower extremities and the thrusting propulsive movements of the legs are transmitted to the body.
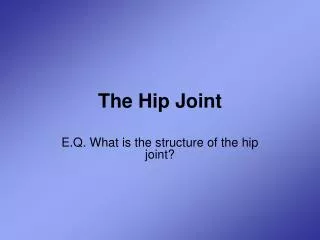
Stability of the hip joint • Closed-packed position: “Max. Stability” Full Extension, slight med. Rotation & Abduction. ”Less Congruency” because ligaments are taut. • Loose-packed position “Min. Stability. Full Congruent” Position: flexion 90, small abduction & small lat. Rotation “Quadruped Position” because ligaments are slack
Stability of the hip joint • The position of greatest risk for dislocation occurs when the hip is flexedand adducted ( sitting with thigh crossed). Mild force along the femoral axis can cause posterior dislocation.
Factors affecting stability of the hip Jt 1- Atmospheric pressure: -ve pressure inside the Jt. 2- Shape of the articulating surface. 3- Labrum acetabular. 4- Direction of the femoral neck. 5- Capsule encircle the femoral neck. 6- Ligaments & Periarticular ms.
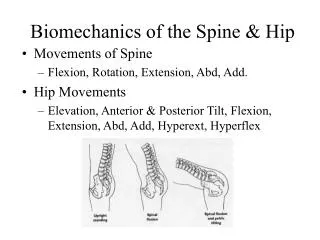
Surface motion of the hip joint • Definition: motion happen at the articular surfaces and can not be observed by the eyes. • From neutral position: Flexion “posterior Spin” & extension “anterior spin”. Opposit direction. • From other position: Flex & Ext, Abd & Add, Med & Lat, rotation. Spinning & Gliding.
Open and Closed chains of the hip joint Open kinematic chain: head and trunk follow the motion of the pelvis. (Lumber-pelvic rhythm) Closed Kinematic Chain: head remains upright. The lumbar spine tends to be the first line of defense in both open and closed kinematic chain of the hip joint.
Lumber-pelvic rhythm A) Lumber pelvic rhythm during trunk flexion ( at hip , pelvis and lumbar spine) aims to increase ROM than might be available to one segment. 45 degrees lumber flexion with trunk inclination) & 90 degrees hip flexion Sequence: flexion of lumbar spine , ant. Pelvic tilt then hip flexion. B) Lumber pelvic rhythm during trunk extension. the reverse. C) “closed kinematic chain” Lumber spine rotate in one direction while the lumber spine rotate in opposite direction
Trunk flexionA)normal rhythm B) limited hip flexion C) limited lumber flexion.
Trunk extensionA) Early phase by extension hip B) Middle phase occurs by extension of lumbar spine C) In last phase the muscle activity reduced.
Weight transmission through the hip joint • Major Trabecular systems 1-Medial trabecular system “compression” 2-Lateral trabecular system “shearing & tensile” • Minor Trabecular system 1-Medial accessory 2-Lateral accessory
Kinetic • Static: 1- Bilateral stance : symmetrical & asymmetrical. 2- Unilateral stance • Dynamic: Two peak forces the 1st (4w) just after heel strike, the 2nd (7w) just before toe off (Abductor ms).
Statics: bilateral Standing • A- In the sagittal plane: LOG falls just posterior to the hip joint axis (extension moment) checked by passive tension in the ligaments & joint capsule. • B- In the frontal plane: the weight of the HAT equals 2/3 of BW (1/3 for each hip).
Statics: Transverse stability of the pelvis: • A- Symmetrical bilateral standing : no muscle activity is needed. • B- Asymmetrical bilateral standing : simultaneous contraction of the ipisilateral and contralateral abductors and adductors to restore balance.
Statics: unilateral Standing • Stance hip carries 5/6 (4/6 w. of HAT + ¼ w. of the other LE) of total BW (820 N.)
Reduction of joint reaction force: Importance: If the hip joint undergoes osteoarthritic changes leading to pain on weight bearing, the JRF must be reduced to avoid pain. Several strategies could be used: 1- Weight loss: Reduce of 1N of body weight will reduce JRF 3N. Example: if the patient lost 10kg, so the JRF will be reduced by …….. N.
Reduction of joint reaction force: 2- Reduction of abductor muscle force: This could be achieved by reducing the moment arm of the gravitational force through lateral leaning of trunk towards the side of pain or weakness. • If the lateral trunk lean is due to hip abductor weakness, gait is called gluteus medius gait. • If it is due to hip joint pain , gait is called antalgic gait.
Reduction of joint reaction force: • 3- using the cane ipsilaterally and contralaterally: • Ipisilateral: provide some benefits in energy expenditure by reducing the BW by the amount of downward thrust • Yet, lateral trunk lean is more effective in reducing JRF than using the cane ipsilaterally .
Reduction of joint reaction force: • Contralaterally: relieves the hip joint of 60% of its load in stance. • Equation of equilibrium will be as follow: Abductor muscle torque + cane torque (latissimus dorsi) = Gravitational torque.
Dynamics • Two peak forces • The 1st (4w) just after heel strike, • The 2nd (7w)just before toe off (Abductor ms).
Pathomechanics (1)- Bone abnormality: A) Neck shaft angle: - Coxa Valga - Coxa Vara B) Angle of torsion: Excessive Anteversion Toe-in gait Retroversion Toe-out gait
Neck Shaft AngleCoxa Valga • 1-Decrease bending moment arm. 2-Decrease shear across the femoral neck. 3- decrease the hip abductor moment arm. 4-Increase the demand on the hip abductors. • 5-Increasing JRF. 6-Increases the amount of articular surface exposed superiorly superior dislocation. 7- decrease stability.
Coxa Vara • 1-Increase bending moment arm. 2-Increase shear across the femoral neck( increased density of lateral trabecular system due to increased tensile forces + increased liability of femoral neck fracture in adults and slipped capital femoral epiphysis. 3- Increase the hip abductor moment arm. 4-Decrease the demand on the hip abductors. • 5-Decrease JRF. 6-Decrease the amount of articular surface exposed superiorly with decreased liability of superior dislocation. 7- Increase stability.
Angle of torsion • Excessive Anteversion: • - Femoral head twisted anteriorly increasing the amount of anterior articular surface exposure predisposing to anterior dislocation. • -Subject will walk with toe-in gait to restore stability. • -Decrease abductor muscle moment arm. • -Increase demand on hip abductors. • -Increase JRF.
Retroversion • - Femoral head twisted Posterior decreasing the amount of anterior articular surface exposure • -Subject will walk with toe-out gait to restore mobility. • -Increase abductor muscle moment arm. • -Decrease demand on hip abductors. • -Decrease JRF.