Download
1 / 21
290 likes | 1.39k Views
Case 1:. 3 year-old boy presented at age 2 years-old with recurrent fever and pharyngitis which started 5 months of ageNormal growthStrep negative, primary immunodeficiency ruled-outStarted prednisone for presumed PFAPA with good response; however, continued to have monthly fevers requiring predn

E N D
1. Periodic Fever with Aphthous Stomatitis, Pharyngitis, and Adenitis (PFAPA) Mark Cody Smith, MD
West Virginia University
Department of Pediatrics
March 23, 2012
2. Case 1: 3 year-old boy presented at age 2 years-old with recurrent fever and pharyngitis which started 5 months of age
Normal growth
Strep negative, primary immunodeficiency ruled-out
Started prednisone for presumed PFAPA with good response; however, continued to have monthly fevers requiring prednisone
Tonsillectomy at age 2 years of age, asymptomatic since
Every time he was taken to the dr or ER where numerous tests were obtained, and everytime the patient was placed on an antibiotics.
His immunologic evaluation included ALC, Immunoglobulins, lymphocyte subsets, specific antibody response and CH 50. Every time he was taken to the dr or ER where numerous tests were obtained, and everytime the patient was placed on an antibiotics.
His immunologic evaluation included ALC, Immunoglobulins, lymphocyte subsets, specific antibody response and CH 50.
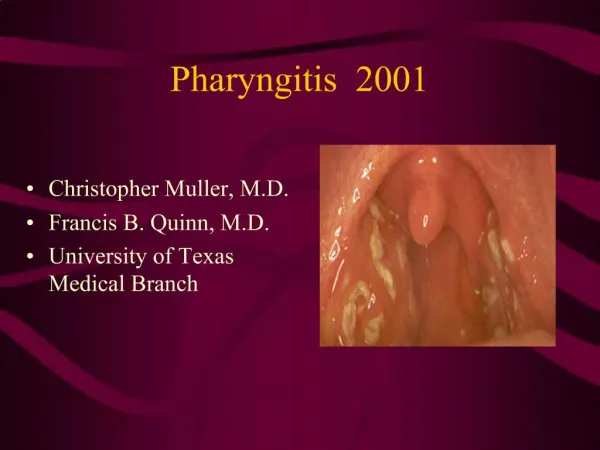
3. Pharyngitis:
4. Aphthous Ulcers:
5. Case 2: 2 year-old girl presented with cervical lymphadenitis and fevers that occurred every 21 days since age 6 months
Normal growth
Strep negative throat cultures, primary immunodeficiency ruled-out
Never neutropenic
Asymptomatic after 1 dose of prednisone This girl also required numerous dr or ER visit and numerous blood and urine tests as well as throat culture and blood culture.
Cyclic neutropenia had to be ruled out due to every 21-day symptoms, and it�s treatment is completely different.This girl also required numerous dr or ER visit and numerous blood and urine tests as well as throat culture and blood culture.
Cyclic neutropenia had to be ruled out due to every 21-day symptoms, and it�s treatment is completely different.
6. Case 3: 3 year-old boy presented with monthly fevers and pharyngitis since age 5 months
Normal growth
Multiple negative throat cultures
CBC with elevated inflammatory markers and elevated neutrophils during febrile episode
Labs normalized between fever episodes
Fevers resolved after just 1 dose of prednisone Multiple Dr. and ED visits for fevers and sore throats. Had multiple set of basic labs drawn and received multiple courses of antibiotics.Multiple Dr. and ED visits for fevers and sore throats. Had multiple set of basic labs drawn and received multiple courses of antibiotics.
7. Case 4:
8. Introduction: PFAPA is an auto-inflammatory recurrent fever syndrome.
Incidence unknown
Unknown cause
Elevations of several inflammatory cytokines suggest a primary problem in the innate immune system
Benign and self-limited with no long term sequelae
Abrupt onset of fever (38.9�C-41.1�C) for 3-6 days occurring an average of every 28 days
- First described in 1987 by Marshall et al. Sometimes referred to as Marshall syndrome
- Elevated cytokines include tumor necrosis factor alpha, interleukin-6 and -8, and interferon gamma.
- Monocytes are often increased and eosinophils and lymphocytes are often decreased during fevers.- First described in 1987 by Marshall et al. Sometimes referred to as Marshall syndrome
- Elevated cytokines include tumor necrosis factor alpha, interleukin-6 and -8, and interferon gamma.
- Monocytes are often increased and eosinophils and lymphocytes are often decreased during fevers.
9. Epidemiology: 2-5 years of age
Slight male predominance (55-71%)
Familial cases rare
No ethnic or racial group predilection
Attacks occur less often after age 5 years of age and typically cease prior to 10 years of age
10. Diagnostic Criteria: > 3 episodes of fever between 3-6 week intervals lasting no more than 5 days (identical symptoms)
Pharyngitis + tender cervical lymphadenitis or aphthous ulcers
Normal growth
Rapid symptoms resolution with a single dose of prednisone Diagnosis of exclusion � primary immune deficiency, cyclical neutropenia, etc.Diagnosis of exclusion � primary immune deficiency, cyclical neutropenia, etc.
11. Exclusion Criteria: Neutropenia
Atypical symptoms
Cough, coryza, diarrhea, rash, arthritis, severe abdominal pain, or neuromuscular symptoms
Elevated acute phase reactants between attacks
Family history of recurrent fever
12. Differential Diagnosis: Cyclical neutropenia
21 day cycles, gingival disease
Hyper-IgD syndrome
Familial Mediterranean fever
TNF receptor 1 associated periodic syndrome (TRAPS)
Muckle-Wells syndrome
Infectious disease or malignancy rarely diagnosed if predictable periodic fever
Primary reason for accurate diagnosis is to relieve parental anxiety Each of the second group has a different characteristic symptom pattern.Each of the second group has a different characteristic symptom pattern.
13. Treatment: Goal
Curtail aberrant immune response
Expectant Management
Treatment is optional given the favorable natural history
Glucocorticoids
Cimetidine
Colchicine
not recommended
Tonsillectomy +/- adenoidectomy
14. Treatment: Glucocorticoids- 1st line
Prednisone/Prednisolone
1 -2 mg/kg/dose at onset of fever, may need to repeat
Quick response (within hours)
May increase frequency of attacks
Most common adverse effects- restlessness and sleep disruption (give > 4 hours prior to bedtime)
Ulcers last to resolve
15. Treatment: Cimetidine- 2nd line
20-40 mg/kg/day divided q12h
May need to divide up to 4 times daily- adherence?
If works, continue for 6 months before stopping
Tonsillectomy +/- adenoidectomy:
Controversial because benign/self-limited condition
Effective in most patients
Reserved for those who failed conservative therapy
Experimental:
Anakinra- recombinant IL-1 receptor antagonist
Promising potential line of treatment
Cost? Availability?
16. Summary: PFAPA should be considered in young children with cyclical fevers and streptococcal negative pharyngitis
Benign, self-limited condition diagnosed clinically
Primary reason for accurate diagnosis is to relieve parental anxiety
17. Summary: Strict adherence to diagnostic criteria will reasonably exclude more serious conditions
May need to rule-out cyclical neutropenia based on history (21 day cycle)
Prednisone if 1st line therapy and may be diagnostic
18. Acknowledgment: I would like to thank Dr. Yesim Demirdag for her wisdom and guidance.
19. Thank You!
20. Sources: Reiman HA. Periodic disease: a probably syndrome including periodic fever, benign paroxysmal peritonitis, cyclic neutropenia and intermittent arthralgia. JAMA 1948; 136:239.
Stojanov S, Kastner DL. Familial autoinflammatory diseases: genetics, pathogenesis and treatment. Curr Opin Rheumatol 2005; 17:586.
Marshall GS, Edwards KM, Butler J, Lawton AR. Syndrome of periodic fever, pharyngitis, and aphthous stomatitis. J Pediatr 1987; 110: 43�6.
Marshall GS, Edwards KM. PFAPA syndrome (letter). Ped infect Dis J 1989;8:658-9.
Padeh S. Periodic fever syndromes. Pediatr Clin North Am 2005; 52:577.
Feder HM, Salazar JC. A clinical review of 105 patients with PFAPA (a periodic fever syndrome). Acta Paediatr 2010; 99:178.
Sampaio IC, Rodrigo MJ, Monteiro Marques JG. Two siblings with periodic fever, aphthous stomatitis, pharyngitis, adenitis (PFAPA) syndrome. Pediatr Infect Dis J 2009; 28:254.
Adachi M, Watanabe A, Nisheiyama A, et al. Familial cases of periodic fever with aphthous stomatitis, pharyngitis, and cervical adenitis syndrome. J Pediatr 2011; 158:155.
21. Sources: 9. Valenzuela PM, Majerson D, Tapia JL, Talesnik E. Syndrome of periodic fever aphthous stomatitis, pharyngitis, and adenitis (PFAPA) in siblings. Clin Rheumatol 2009; 28:1235.
10. Stojanov S, Hofmann F, Kery A, et al. Cytokine profile in PFAPA syndrome suggests continuous inflammation and reduced anti-inflammatory response. Eur Cytokine Netw 2006; 17:90.
11. Stojanov S, Lapidus S, Chitkara P, et al. Periodic fever, aphthous stomatitis, pharyngitis, and adenitis (PFAPA) is a disorder of innate immunity and Th1 activation responsive to IL-1 blockade. Proc Natl Acad Sci USA 2011; 108:7148.
12. Brown KL, Wekell P, Osla V, et al. Profile of blood cells and inflammatory mediators in periodic fever, aphthous stomatitis, pharyngitis and adenitis (PFAPA) syndrome. BMC Pediatr 2010; 10:65.
13. Thomas KT, Feder HM Jr, Lawton AR, Edwards KM. Periodic fever syndroms in children. J Pediatr 1999; 135:15.
14. Kovacs L, Hlavata A, Baldovic M, et al. Elevated immunoglobulin D levels in children with PFAPA syndrome. Neuro Endocrinol Lett 2010; 31:743.
15. Pedeh S, Sheba Medical Center, personal communication, 2010.
16. Burton MJ, Pollard AJ, Ramsden JD. Tonsillectomy for periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis syndrome (PFAPA) (Review). The Cochrane Lib 2010; 9:1-17.