Download
1 / 54
540 likes | 1.41k Views
Assessment of Digestive and Gastrointestinal Function Part 1. Second Semester 2ed Years students Miss Iman shaweesh January 2008. ANATOMY OF THE GASTROINTESTINAL TRACT.

E N D
Assessment of Digestive andGastrointestinal FunctionPart 1. Second Semester 2ed Years students Miss Imanshaweesh January 2008
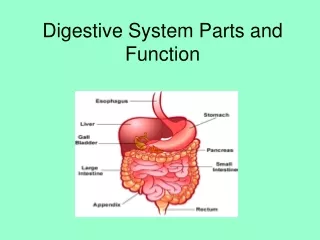
ANATOMY OF THEGASTROINTESTINAL TRACT • GI tract is a 23- to 26-foot-long pathway that extends from the mouth through the esophagus, stomach, and intestines to the anus The esophagus is located in the mediastinum in the thoracic cavity, anterior to the spine and posterior to the trachea and heart. This collapsible tube, which is about 25 cm (10 inches) in length, becomes distended when food passes through it. It passes through the diaphragm at an opening called diaphragmatic hiatus.
The stomach is situated in the upper portion of the abdomen to the left of the midline, just under the left diaphragm. It is a distensible pouch with a capacity of approximately 1500 mL. The inlet to the stomach is called the esophagogastric junction; it is surrounded by a ring of smooth muscle called the lower esophageal sphincter (or cardiac sphincter), which, on contraction, closes off the stomach from the esophagus.
The stomach can be divided into four anatomic regions: 1- the cardia (entrance), 2- fundus, 3- body, 4- pylorus (outlet).
The small intestine is the longest segment of the GI tract,accounting for about two thirds of the total length. It folds back and forth on itself, providing approximately 7000 cm of surface area for secretion and absorption, the process by which nutrients enter the bloodstream through the intestinal walls. The small intestine is divided into three anatomic parts: the upper part, called the duodenum; the middle part, called the jejunum; and the lower part, called the ileum. The common bile duct which allows for the passage of both bile and pancreatic secretions empties into the duodenum at the ampulla of Vater.
The junction between the small and large intestine, the cecum, is located in the right lower portion of the abdomen. The ileocecal valve is located at this junction. It controls the passage of intestinal contents into the large intestine and prevents reflux of bacteria • The vermiform appendix is located near this junction.
The large intestineconsists of an ascending segment on the right side of the abdomen, a transverse segment that extends from right to left in the upper abdomen, and a descending segment on the left side of the abdomen. The terminal portion of the large intestine consists of two parts: the sigmoid colon and the rectum. The rectum is continuous with the anus.
The GI tract receives blood from arteries that originate along the entire length of the thoracic and abdominal aorta. • Of particular importance are the gastric artery and the superior and inferior mesenteric arteries. • Oxygen and nutrients are supplied to the stomach by the gastric artery and to the intestine by the mesenteric arteries
Blood is drained from these organs by veins that merge with others in the abdomen to form a large vessel called the portal vein. Nutrient-rich blood is then carried to the liver. The blood flow to the GI tract is about 20% of the total cardiac output and increases significantly after eating. Both the sympathetic and parasympathetic portions of the autonomic nervous system innervate the GI tract. In general, sympathetic nerves exert an inhibitory effect on the GI tract, decreasing gastric secretion and motility and causing the sphincters and blood vessels to constrict.
Parasympathetic nerve stimulation causes peristalsis and increases secretary activities. The sphincters relax under the influence of parasympathetic stimulation. The only portions of the tract that are under voluntary control are the upper esophagus and the external anal sphincter.
FUNCTION OF THE DIGESTIVE SYSTEM • All cells of the body require nutrients. These nutrients are derived from the intake of food that contains proteins, fats, carbohydrates, vitamins and minerals, and cellulose fibers and other vegetable matter of no nutritional value. The primary digestive functions of the GI tract are the following: • To break down food particles into the molecular form for digestion
To absorb into the bloodstream the small molecules produced by digestion • To eliminate undigested and unabsorbed foods tuffs and other waste products from the body • After food is ingested, it is propelled through the GI tract, coming into contact with a wide variety of secretions that aid in its digestion, absorption, or elimination from the GI tract.
Chewing and Swallowing • The process of digestion begins with the act of chewing, in which food is broken down into small particles that can be swallowed and mixed with digestive enzymes. Eating—or even the sight,smell, or taste of food—can cause reflex salivation. Saliva is secreted from three pairs of glands: the parotid, the submaxillary, and the sublingual glands. Approximately 1.5 L of saliva is secreted daily. Saliva is the first secretion that comes in contact with food. Saliva contains the enzyme ptyalin, or salivary amylase, which begins the digestion of starches
Swallowing begins as a voluntary act that is regulated by a swallowing center in the medulla oblongata of the central nervous system. • As food is swallowed, the epiglottis moves to cover the tracheal opening and prevent aspiration of food into the lungs. Swallowing, which propels the bolus of food into the upper esophagus, thus ends as a reflex action.
The smooth muscle in the wall of the esophagus contracts in a rhythmic sequence from the upper esophagus toward the stomach to propel the bolus of food along the tract. During this process of esophageal peristalsis, the lower esophageal sphincter relaxes and permits the bolus of food to enter the stomach. • Subsequently, the lower esophageal sphincter closes tightly to prevent reflux of stomach contents into the esophagus.
Gastric Function • The stomach stores and mixes the food with secretions. It secretes a highly acidic fluid in response to the presence or anticipated ingestion of food. This fluid, which may have a pH as low as 1, derives its acidity from the hydrochloric acid (HCl) secreted by the glands of the stomach.
The function of this gastric secretion is two-fold: • to break down food into more absorbable components. • to aid in the destruction of most ingested bacteria. • The stomach can produce about 2.4 L per day of these gastric secretions. Gastric secretions also contain the enzyme pepsin, which is important for initiating protein digestion.
Intrinsic factor is also secreted by the gastric mucosa. This compound combines with dietary vitamin B12 so that the vitamin can be absorbed in the ileum.
Peristaltic contractions in the stomach propel its contents toward the pylorus. Because large food particles cannot pass through the pyloric sphincter, they are churned back into the body of the stomach. In this way, food in the stomach is agitated mechanically and broken down into smaller particles. • Food remains in the stomach for a variable length of time, from a half-hour to several hours, depending on the size of food particles, the composition of the meal, and other factors.
This food mixed with gastric secretions is called chyme. Hormones, neuroregulators, and local regulators found in the gastric secretions control the rate of gastric secretions and influence gastric motility
Small Intestine Function • The digestive process continues in the duodenum. Secretions in the duodenum come from the accessory digestive organs—the pancreas, liver, and gallbladder—and the glands in the wall of the intestine itself. These secretions contain digestive enzymes and bile.
Pancreatic secretions have an alkaline pH because of high concentrations of bicarbonate. This neutralizes the acid entering the duodenum from the stomach. • The pancreas secretes enzymes, including 1- trypsin, which aids in digesting protein; 2- amylase- digesting starch; and 3- lipase, aids in digesting fats
Bile (secreted by the liver and stored in the gallbladder) aids in emulsifying ingested fats, making them easier to digest and absorb. The intestinal glands secrete mucus, hormones, electrolytes, and enzymes. • Intestinal secretions total approximately 1 L/day of pancreatic juice, 0.5 L/day of bile, and 3 L/day of secretions from the glands of the small intestine.
Colonic Function • Within 4 hours after eating, residual waste material passes into the terminal ileum and passes slowly into the proximal portion of the colon through the ileocecal valve. • This valve, which is normally closed, helps prevent colonic contents from refluxing into the small intestine. With each peristaltic wave of the small intestine, the valve opens briefly and permits some of the contents to pass into the colon. • Bacteria make up a major component of the contents of the large intestine. They assist in completing the breakdown of waste material, especially of undigested or unabsorbed proteins and bile salts.
Waste Products of Digestion • Feces consist of undigested foodstuffs, inorganic materials, water, and bacteria. Fecal matter is about 75% fluid and 25% solid material. • The composition is relatively unaffected by alterations in diet, because a large portion of the fecal mass is of nondietary origin, derived from the secretions of the GI tract. The brown color of the feces results from the breakdown of bile by the intestinal bacteria. Chemicals formed by intestinal bacteria (especially indole and skatole) are responsible in large part for the fecal odor.
Waste Products of Digestion • Gases formed contain methane, hydrogen sulfide, and ammonia, amongothers. The GI tract normally contains approximately 150 mL of these gases, which are either absorbed into the portal circulation and detoxified by the liver or expelled from the rectum as flatus.
Waste Products of Digestion • Elimination of stool begins with distention of the rectum, which reflexively initiates contractions of the rectal musculature and relaxes the normally closed internal anal sphincter. The internal sphincter is controlled by the autonomic nervous system; the external sphincter is under the conscious control of the cerebral cortex. During defecation, the external anal sphincter voluntarily relaxes to allow colonic contents to be expelled. Normally, the external anal sphincter is maintained in a state of tonic contraction. Thus, defecation is seen to be a spinal reflex (involving the parasympathetic nerve fibers) that can be inhibited voluntarily by keeping the external anal sphincter closed.
AssessmentHEALTH HISTORY ANDCLINICAL MANIFESTATIONS • Pain Pain can be a major symptom of GI disease. The character, duration,pattern, frequency, location, distribution of referred pain and time of the pain vary greatly depending on the underlying cause. Indigestion: Upper abdominal discomfort or distress associated with eating (commonly called indigestion) is the most common symptom of patients with GI dysfunction.
Indigestion • result from disturbed nervous system control of the stomach or from a disorder in the GI tract or elsewhere in the body. Fatty foods tend to cause the most discomfort, because they remain in the stomach longer than proteins or carbohydrates do.
Intestinal Gas - accumulation of gas in the GI tract may result in belching (the expulsion of gas from the stomach through the mouth) or flatulence (the expulsion of gas from the rectum). • Nausea and Vomitingnausea, which can be triggered by odors, activity, or food intake. The emesis, or vomitus, may vary in color and content. It may contain undigested food particles or blood (hematemesis). • Change in Bowel Habits and Stool Characteristics
Stool is normally light to dark brown.the ingestion of certain foods and medications, can change the appearance of stool
PHYSICAL ASSESSMENT • includes assessment of the mouth, abdomen, and rectum. The mouth, tongue, buccal mucosa, teeth, and gums are inspected, and ulcers, nodules, swelling, discoloration, and inflammation are noted. People with dentures should remove them during this part of the examination to allow good visualization. • The patient lies supine with knees flexed slightly for inspection, auscultation, palpation, and percussion of the abdomen
Diagnostic Evaluation • Common blood tests include (CBC), carcinoembryonic antigen (CEA),liver function tests, serum cholesterol, and triglycerides. Test findings may reveal alterations in basal metabolic function and mayindicate the severity of a disorder. • The preparation for many of these studies (endoscopy or GI laboratory). includes fasting, the use of laxatives or enemas, and ingestion or injection of a contrast agent or a radiopaque dye.
General nursing interventions for the patient who is having GI diagnostic assessment include the following: • Providing general information about a healthy diet and the nutritional factors that can cause GI disturbances; after a diagnosis has been confirmed. • Providing needed information about the test and the activities required of the patient. • Providing instructions about postprocedure care and activity restrictions
Alleviating anxiety . • Helping the patient cope with discomfort • Encouraging family members or others to offer emotional. • support to the patient during the diagnostic testing • Assessing for adequate hydration before, during, and immediately after the procedure, and providing education about maintenance of hydration
STOOL TESTS • BREATH TESTS The hydrogen breath test was developed to evaluate carbohydrate absorption. It also is used to aid in the diagnosis of bacterial overgrowth in the intestine and short bowel syndrome. This test determines the amount of hydrogen expelled in the breath after it has been produced in the colon
Urea breath tests detect the presence of Helicobacter pylori, the bacteria that can live in the mucosal lining of the stomach and cause peptic ulcer disease. The patient takes a capsule of to 20 minutes later. • ABDOMINAL ULTRASONOGRAPHY • Endoscopic ultrasonography (EUS) is a specialized enteroscopic procedure that aids in the diagnosis of GI disorders by providing direct imaging of a target area.
DNA TESTING • Researchers have refined methods for genetic risk assessment, preclinical diagnosis, and prenatal diagnosis to identify persons who are at risk for certain GI disorders (eg, gastric cancer, lactose deficiency, inflammatory bowel disease, colon cancer). In some cases, DNA testing allows practitioners to prevent (or minimize)
IMAGING STUDIES • Imaging studies include x-ray and contrast studies, computed tomography (CT) scans, magnetic resonance imaging (MRI), and scintigraphy (radionuclide imaging). • Upper Gastrointestinal Tract Study • Lower Gastrointestinal Tract Study • Gastrointestinal Motility Studies
ENDOSCOPIC PROCEDURES • Fiberscopes are flexible scopes equipped with fiberoptic lenses. Fibroscopy of the upper GI tract allows direct visualization of the esophageal, gastric, and duodenal mucosa through a lighted endoscope (gastroscope NSG Intervention • The patient should not eat or drink for 6 to 12 hours before the examination
NSG Intervention • Patient preparation includes helping the patient spray or gargle with a local anesthetic, and administering midazolam (Versed) intravenously just before the scope is introduced. • Midazolam is a sedative that provides moderate sedation and relieves anxiety during the procedure • The nurse positions the patient on the left side to facilitate saliva drainage and to provide easy access for the endoscope.