Download
1 / 5
50 likes | 180 Views
The Fun and Easy Guide to Posters. 1. Prepare poster as a single power point slide or Adobe PDF file, following and improving the attached templates 2. Copy poster to a diskette or CD

E N D
The Fun and Easy Guide to Posters 1. Prepare poster as a single power point slide or Adobe PDF file, following and improving the attached templates 2. Copy poster to a diskette or CD 2b. Note the poster should be in landscape mode and sized as 56 x 35 inches (you can specify 17 X 22 later and select “scale to print paper” to get a smaller size) 3. Bring Poster to room 501 in 6116. Print Poster on the Large Format Printer, following the posted instructions Details on Next Page
Poster Printing General Information • On site monitoring 8 am – 5:30 pm weekdays • Access from Windows or Mac • For setup or troubleshooting contact the Help Desk at 301-496-0268 • HP DesignJet 1055CM plus • Mac – AppleTalk 41/HPDesignJet 1055CM1 • Windows – network printque b616_dj1055 • Turn off background printing for large (>10 mb files) • Please limit drafts Printing a poster Graphics software: • Adobe products and MS PowerPoint work well. • PowerPoint is available free of charge. Adobe products are purchased at a significant discount. Contact the Help Desk for assistance acquiring either. Printing in PowerPoint: In Page Setup • Make the “Slides sized for” box Custom • Change the width to your desired width (56” maximum) and height to no more than 35.5”. Change orientation to landscape Insert graphics as JPEG format to limit document size. Printing in Adobe products: In Print Setup • Select page size closest to what you need (typically 36 by 60) and a landscape orientation. In the Document Setup check the “Use Print Setup” box. Save the document in PDF format. Helpful Tips & Web resources • Print early in the day. During heavy use, waiting time for the printer can be 2 hours or more. • Give yourself plenty of time. Posters are complex. • Print larger posters (10 or more Mb) with background printing turned off. • Print a handout version (8.5” x 11”) of your poster on your own printer first. • Use a white background for faster printing. • Use printer friendly fonts (eg Ariel, Helvetica, Times) • For “photo quality graphics,” print images on a photoprinter and affix them to the poster. • For Macs: Donʼt forget to reset your chooser back to your normal printer after printing a poster. • NIH Medical Arts and Photography Branch (MAPB) provides professional design and print services – 301-496-5995 • Helpful resources on the web for poster design/presentation: http://www.ncsu.edu/project/posters/ http://www.scifor.com/Guidelines.htm http://www.ees.nmt.edu/posters.html http://www.swarthmore.edu/NatSci/cpurrin1/posteradvice.html The website addresses are provided as a courtesy. NIH and NCI are not responsible for content.
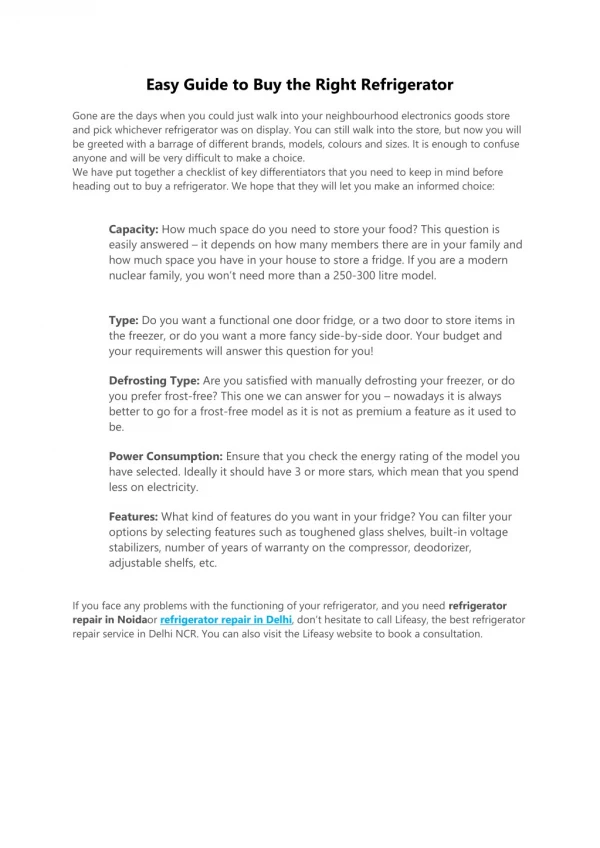
Distress and BRCA1/2 Testing: The Role of Physical Activity Ashley W. Smith, Ph.D., M.P.H.1 & Andrew Baum, Ph.D.2 1Cancer Prevention Fellow, Division of Cancer Prevention, NCI 2Behavioral Medicine Oncology, University of Pittsburgh Cancer Institute Physical Activity & Psychological Response Abstract Background: Research has shown physical and psychological benefits of exercise across the cancer experience. There is extensive evidence suggesting that physical activity is associated with lower levels of distress and better quality of life among cancer survivors. However, few studies have examined the effects of physical activity on those at high cancer risk. More specifically, research examining the effects of physical activity during stress associated with genetic testing is lacking. Purpose: The current study investigated associations between physical activity level and self-reported distress before and after BRCA1/2 genetic testing. Methods:Participants included 131 women (68 breast and ovarian cancer survivors, 63 women with a breast cancer family history) considering genetic testing. Of those, 23 decided not to be tested, 22 tested positive, 73 tested negative, and 13 received variant results. Data were obtained through questionnaires administered prior to BRCA1/2 genetic testing, after receiving results, and at a 3-month follow-up visit. Results: Distress dissipated in all participants over time, with no significant differences based on test results. However, individuals with a personal cancer history reported higher levels of distress. Sedentary individuals reported more depressive symptoms before and after testing, compared with those who were consistently active or those who reported at least 2½ hours of activity per week. The relationship between higher activity and fewer depressive symptoms continued to be significant even after controlling for age, cancer status and related treatment, test results, and psychiatric medication use. Conclusion: Results suggest a robust relationship between increased physical activity and lower distress in women undergoing BRCA1/2 testing, although the causal direction of this relationship cannot be determined. These data indicate the need for randomized intervention studies evaluating physical activity programs for women at high risk of breast and ovarian cancer. • Measurement • Questionnaire Assessments • Pre-Test: Prior to Genetic testing • Post-Test: Within 1 week of receiving test results • Follow-up: 3 months after Post-Test Pre-test Activity Level & Depression (CESD): High active participants had fewer depressive symptoms than Sedentary p<.05 Predictor Measures • Cancer History • Testing Status/Results • Physical Activity Level 1. By CDC criteria: Sedentary; Low (<150 min/wk); High (>150 min/wk) 2. By number of time points active Outcome Measures • Physical Activity (self-reported minutes of activity per week) • Distress: 1. Depressive symptoms (CES-D; SCL90R) 2. Anxiety (STAI; SCL-90R) 3. Global Distress symptoms (SCL90R GSI) Cross-Sectional Physical Activity at each Time Point Physical Activity Consistency & Depression (CESD): ConsistentlyActive participants had fewer depressive symptoms than Consistently Sedentary 36-40% met CDC activity goals at each time point, but only 24% met goals at all time points • Background Breast/Ovarian Cancer Risk • Breast Cancer is the most common cancer in American women • Ovarian Cancer causes more deaths than any other female reproductive cancer • Both have better prognosis if identified and treated early • Screening for BRCA1 and BRCA2 genes provides enhanced surveillance but health care professionals and women at higher familial risk must now decide when it is appropriate to test • Psychological Effects of Breast/Ovarian Cancer Risk • First degree relatives report more distress • Worry about Breast Cancer is associated with increased surveillance • Research on the psychological response to BRCA1/2 testing has been mixed • Interest in BRCA1/2 testing is associated with distress and those most likely to request testing may be more psychologically vulnerable Physical Activity Goals and Psychological Effects • CDC has set U.S. physical activity goal to 2½ hrs (150 min.) per week for health benefits • Physical Activity is associated with decreased risk of some cancers • Physical Activity is associated with lower distress in healthy individuals • Cancer survivors who are more active report lower distress, better quality of life • Very little data is available describing physical activity patterns in those at high risk • No research has examined effects of physical activity during ongoing stress associated with genetic testing p<.05 Physical Activity Consistency & SCL90R: ConsistentlyActive participants had less general distress and fewer depressive symptoms than Consistently Sedentary Psychological Responses over Time p=.001 Depressive Symptoms (CESD) decreased at Follow-Up Anxiety (STAI) Decreased over Time p<.01 p<.05 p<.001 Study Goals Psychological: To examine the psychological effects of BRCA1/2 gene testing Physical Activity: To categorize physical activity in women considering BRCA1/2 gene testingbased on public health recommendations Stress-Buffering: To determine whether physical activity is associated with reduced distress in women considering BRCA1/2 gene testing p<.05 • Conclusions • Activity levels were comparable to U.S. and high risk samples: 27% were sedentary at every time point and 24% met U.S. activity goal at all time points • All participants reported less distress post-test and 3-months later; Cancer survivors reported more general distress symptoms and more anxiety on the SCL-90 anxiety subscale than those with no history of cancer (Not Shown) • There were no significant differences in distress by testing status or results • Those with higher or more consistent activity levels reported fewer depressive symptoms than sedentary participants, even after controlling for age, cancer status, recency of diagnosis & treatment, and psychiatric medication use • Limitations included small sample size, correlational findings, and a limited physical activity measurement • Findings suggest that interventions are needed to increase activity levels to reach U.S. public health goals and that physical activity is associated with lower distress in individuals undergoing BRCA1/2 testing Participants General Distress (SCL90R GSI) Decreased Pre-Post Test Anxiety (SCL90R) marginally decreased at 3 months Cancer Status: • Unaffected, at high risk (n=68) • Current/History of Cancer (n=63) Stage: • O (n=8) • I or II (n=57) • III (n=6) Treatment: • Chemotherapy (n=12) • Radiation (n=6) Age: 22-70 (mean = 45 yrs) Ethnicity:Caucasian Education: 83% college/graduate degree BRCA1/2 Results: • No test (n=23) • Positive (n=22) • Negative (n=73) • Variant (n=13) p<.05 p=.05
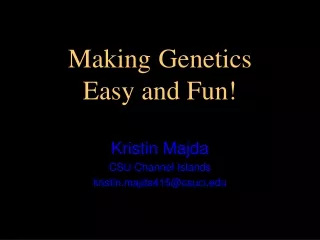
Tamoxifen Net Benefit for White Women Tamoxifen Eligibility for White Women Risk Factor Category Relative Risk of IBC, next 5 y Age Group in Years Age Group in Years Total Number Total Number Number Benefiting from Tamoxifen Number Benefiting from Tamoxifen % Benefiting from Tamoxifen (95% CI) % Benefiting from Tamoxifen (95% CI) Age at menarche, y >14 > 12-13 < 12 1.00 1.10 1.21 35-79 50,104,829 2,431,911 4.9% (4.4% to 5.4%) 35-79 50,104,829 9,377,715 18.7% (17.8% to 19.7%) No. of breast biopsies Age at counseling, < 50 y old 0 1 > 2 1.00 1,70 2.88 35-39 7,906,861 0 0.0% (0.0% to 0.3%) 35-39 7,906,861 0 0.0% (0.0% to 0.3%) No. of breast biopsies Age at counseling, > 50 y old 0 1 > 2 1.00 1.27 1.62 40-49 15,577,412 1,263,824 8.1% (6.8% to 9.4%) 40-49 15,577,412 831,199 5.3% (4.2% to 6.4%) 50-59 11,699,803 996,231 8.5% (7.2% to 9.8%) 50-59 11,699,803 1,803,782 15.4% (13.5% to 17.3%) Age at first live birth Number of first-degree relatives with IBC 60-69 7,979,454 163,667 2.1% (1.3% to 3.0%) 60-69 7,979,454 3,008,966 37.7% (34.9% to 40.6%) < 20 years 0 1 > 2 1.00 2.61 6.80 70-79 6,941,299 8,189 0.1% (0.0% to 0.4%) 70-79 6,941,299 3,733,768 53.8% (50.5% to 57.0%) 20-24 years 0 1 > 2 1.24 2.68 5.78 25-29 years or nulliparous 0 1 > 2 1.55 2.76 4.91 Tamoxifen Eligibility, Net Benefit and Use for Breast Cancer Chemoprevention among White Women in the United States. Freedman AN1, Graubard BI2, Rao RS2, McCaskill-Stevens W3, Ballard-Barbash R1, Gail MH2. 1Division of Cancer Control and Population Sciences, 2Division of Cancer Epidemiology and Genetics, 3Division of Cancer Prevention, National Cancer Institute, Bethesda MD, Introduction Methods Results The Breast Cancer Prevention Trial (BCPT), a randomized, placebo-controlled study of the chemopreventive effects of tamoxifen showed a 49% reduction in the risk of invasive breast cancer in a population of women who had an elevated risk of breast cancer. Unfortunately, some women in the trial also experienced adverse outcomes associated with tamoxifen use, including excesses of endometrial cancer, pulmonary embolism, stroke, deep vein thrombosis, and cataracts. To fully understand the public health implications of the BCPT results for the use of tamoxifen for breast cancer chemoprevention in the U.S. population, both the adverse events and proven benefits must be taken into account. Figure 2. Estimates of the percentage of white U.S. women who would be eligible for tamoxifen and the percentage who would have a positive benefit/risk index for tamoxifen chemoprevention, by age Determining Tamoxifen Eligibility The FDA approved indications for tamoxifen chemoprevention age 35 years or older and a 5-year risk of invasive breast cancer of at least 1.67% is based on the Gail Breast Cancer Risk Assessment Model. (http://www.fda.gov/cder/news/tamoxifen/default.htm) We calculated the number of white women, by age, who matched these criteria and would be eligible for tamoxifen chemoprevention by applying those 5-year projected breast cancer risk estimates to the 2000 NHIS CCM data (Table 2 and Figure 2). Calculating Tamoxifen Benefit/Risk Index Women were first categorized according to their 5-year projected breast cancer risk estimates, by age, and whether they had a uterus. We used a benefit/risk index, which was computed as the: net number of life-threatening events prevented (the total number of invasive breast cancers plus hip fractures minus the total number of endometrial cancers, strokes, and pulmonary embolisms) plus half the net number of serious events prevented (the number of in situ breast cancers minus the number of deep vein thromboses) over a 5-year period. The benefit/risk index for a particular woman depended on age, risk factors for breast cancer, and whether she had a uterus. We then used the net benefit/risk indices presented in Figure 1to calculate the number of white women, aged 3579 years, in these categories who would have a positive benefit/risk index. (See estimates in Table 3 and Figure 2). Although the FDA approved indications for tamoxifen chemoprevention include a 5-year risk of invasive breast cancer of at least 1.67%, we calculated the number of women with a positive net benefit/risk index, even for women with a 5-year risk of invasive breast cancer, of at least 1.50%.We used this lower risk cutoff to include most women aged 35 years or older who could potentially benefit from tamoxifen, even though some would not fulfill FDA approved indications. All estimates, including totals and percentages, were weighted by the NHIS sample weights to the total U.S. population. Standard errors used to compute the 95% confidence intervals (CIs) were estimated to take into account the complex multistage probability sampling design of the NHIS . For all 50,104,829 white women aged 35-79 years in the U.S., 9,377,715 (18.7%, 95% CI 17.8% to 19.7%) would be eligible for tamoxifen chemoprevention on the basis of their age and breast cancer risk factors. 2,431,911 (4.9%, 95% CI 4.3% to 5.4%) would have a positive benefit/risk index for tamoxifen chemoprevention. 70,761 (0.2%, 95% CI 0.1% to 0.3%) reported they were currently taking tamoxifen (without a previous diagnosis of breast cancer). If all 2,431,911 women with an estimated net benefit/risk index took tamoxifen over the next 5 years, and if the risk reduction of 49% reported by the BCPT applies, then 28,492 breast cancers would be prevented, or deferred. Aims To estimate the number of white women in the United States: - who would be eligible for tamoxifen chemoprevention based on FDA approved indications - for whom the benefits of taking tamoxifen for breast cancer risk reduction outweigh the adverse events - who are taking tamoxifen for breast cancer risk reduction Conclusions Table 2. Estimates of the total number of U.S. white women eligible for tamoxifen chemoprevention based on FDA indications, by age groups Although a substantial percentage of white U.S. women (18.7%) would be eligible for breast cancer chemoprevention with tamoxifen based on FDA indications, a much smaller percentage (4.9%) would have an estimatednet benefit based on their age and breast cancer risk factors. Few white women without a previous diagnosis of breast cancer (0.2%) currently use tamoxifen. These data have implications for educating healthcare professionals in evaluating the eligibility, net benefit, and appropriate use of tamoxifen for breast cancer chemoprevention for women in the U.S. population. Methods National Survey Data We used the year 2000 National Health Interview Survey Cancer Control Module (NHIS CCM) to collect information on age, age at first live birth, age at menarche, number of first degree relatives with breast cancer, and the number of benign breast biopsies. We also collected data on the number of women who reported they were currently taking tamoxifen. (http://www.cdc.gov/NCHS/nhis.htm) Assessing Breast Cancer Risk Incorporating these factors into the Gail Breast Cancer Risk Assessment Model (See Table 1), we calculated the 5-year projected breast cancer risk for each of 7,728 white women who were between the ages of 35 and 79 years. (http://cancer.gov/bcrisktool) [Women who reported a previous diagnosis of breast cancer were excluded from the analysis.] Websites Table 3. Estimates of the total number of U.S. white women benefiting from tamoxifen chemoprevention based on FDA indications, by age groups Figure 1. Benefit/risk indices for tamoxifen chemoprevention by level of 5-year projected risk of invasive breast cancer among white women with and without a uterus, by age group Table 1. Relative risks and baseline rates used to estimate the risk of invasive breast cancer (IBC) in the next 5 years in the Gail Model Additional information on estimating the risks and benefits of tamoxifen for breast cancer chemoprevention can be found at the following web sites and articles. http://cancer.gov/bcrisktool--NCI's page and accompanying information for calculating individualized breast cancer risk http://cancer.gov/star--NCI's page for STAR trial information http://www.BreastCancerPrevention.com--The National Surgical Adjuvant Breast and Bowel Project is conducting the STAR trial for NCI. This is their Website about the trial http://www.fda.gov/cder/news/tamoxifen/default.htm--FDA's page about tamoxifen for breast cancer risk reduction http://www.ahrq.gov/clinic/uspstf/uspsbrpv.htm--AHRQ page for USPHSTF recommendations on chemoprevention of breast cancer http://www.nolvadex.com/--Astra Zeneca website for tamoxifen, which includes full labeling information and additional mandated education materials Gail MH, Costantino JP, Bryant J, Croyle R, Freedman L, Helzlsouer K, et al. Weighing the risks and benefits of tamoxifen treatment for preventing breast cancer. J Natl Cancer Inst 1999;91:1829-46 Source: Table 10 and 11 of Gail MH, et al. J Natl Cancer Inst 1999;91:1829-46.
Measurement of Physical Activity 1. Leisure time physical activity (LTPA) was assessed by querying frequency and duration of moderate and vigorous activity. Vigorous “Over the past 30 days, did you do any hard or vigorous activities in your free time for at least 10 minutes that caused HEAVY SWEATING OR LARGE INCREASES IN YOUR BREATHING OR HEART RATE?” “How many times per day, per week or per month did you do this HARD or VIGOROUS activity over the past 30 days?” “On average, about how long did you do these HARD OR VIGOROUS activities each time?” Moderate “Over the past 30 days, did you do any moderate activities in your free time for at least 10 minutes that caused only LIGHT SWEATING OR A SLIGHT TO MODERATE INCREASE IN BREATHING OR HEART RATE? (Frequency and Duration as above) 2. Non-leisure time walking and bicycling (NLTWB) was assessed by querying frequency and duration of walking and bicycling: “Over the past 30 days have you walked or bicycled to or from work, school, or to do errands? “How many times per day, week or month did you do this?” “And on average, about how many minutes did you walk or ride your bike each time?” 30 20 LTPA Combined 10 0 M vs F 18-29 NH >HS vs 300+ vs 70+ White <HS vs vs <100 Latino Inclusion of Non-Leisure Time Walking and Bicycling Reduces Apparent Disparities in Adherence to Recommendations Concerning Physical Activity in Adult Californians Berrigan D.1, Ballard Barbash R.1, Troiano R. P1, McNeel, T2, DiSogra, C3. 1 Applied Research Program, Division of Cancer Control and Population Sciences, National Cancer Institute, Bethesda MD, 2Information Management Services, Inc., Silver Spring, MD, 3 UCLA Center for Health Policy Research, Los Angeles, CA. Abstract Influence of Walking and Bicycling on Adherence to Physical Activity Recommendations Inclusion of Non-Leisure Time Walking & Bicycling Reduces Adherence Differences Among Demographic Groups Despite many health benefits of physical activity (PA), reports suggest that only about half of US adults adhere to PA recommendations and adherence is lower in women, the elderly, less educated/lower income groups, and some minority populations. Such disparities could be due to differences in leisure and non-leisure time PA (LTPA) between these groups. This study reports the prevalence of adherence to PA recommendations with and without the inclusion of non-leisure time walking and bicycling (NLTWB) using the 2001 California Health Interview Survey (n=54,344). We categorized adherence (150 minutes/week of moderate PA, 60 minutes/week of vigorous PA, or a combination totaling 150 minutes/week) with respect to LTPA, NLTWB, or both activities. Walking and bicycling were classified as moderate. Higher levels of LTPA were found among males, Pacific Islanders and non-Hispanic whites, and people that were younger, more educated, or had higher incomes. Inclusion of NLTWB reduced these differences with respect to gender, age, race/ethnicity, education and income. For example, odds ratios from logistic regression comparing adherence in respondents with > HS education vs. < HS education (referent) changed from 3.2 (95% CI, 3.0-3.5) to 1.8 (1.7-2.0) after inclusion of NLTWB. In this poster we illustrate these changes using prevalence data. The results highlight the importance of more complete measurements of PA LTPA NLTWB Combined Adherence Difference (%) 60 Introduction 40 • Physical activity is associated with health benefits, including lower risk of colon and post-menopausal breast cancer • Amount of leisure time physical activity (LTPA) is higher among those who are younger, better educated, or have higher incomes • Differences in physical activity level may be associated with health status disparities among socio-economic groups • Past efforts at quantifying physical activity in epidemiological studies and health behavior surveillance focused on LTPA • Assessment of non-leisure time physical activity (NLTPA) could demonstrate the potential influence of physical activity on health disparities and the importance of measuring NLTPA in future etiological studies 20 0 Comparison Between Extremes AIAN Pacific Asian Black White Latino * Pacific Islanders have a higher level of LTPA than Non-Hispanic Whites, but much smaller numbers % Adherent Based on Leisure Time Physical Activity and Non-Leisure Time Walking and Bicycling Race/Ethnicity Conclusions 60 Adherence (%) Characteristics N Leisure time Non Leisure Time Activity Walking and Biking Total (N) 54344 23054 7962 % (SE) 42.97 (0.3) 15.14 (0.2) Gender Male 22562 51.1 (0.4) 14.6 (0.3) Female 31782 35.3 (0.4) 15.6 (0.3) Age 18-29 8111 52.5 (0.7) 19.1 (0.5) 30-39 10920 43.6 (0.6) 14.2 (0.4) 40-49 12078 43.4 (0.5) 12.8 (0.4) 50-59 9415 40.6 (0.7) 13.0 (0.4) 60-69 6093 35.5 (0.9) 16.5 (0.6) 70+ 7727 27.4 (0.7) 14.4 (0.5) Race/Ethnicity White 36063 48.7 (0.3) 12.1 (0.2) African-American 2714 39.6 (1.3) 16.0 (0.8) Latino 9240 33.1 (0.6) 22.6 (0.6) Asian 3886 35.8 (0.9) 14.2 (0.6) Pacific Islander 211 53.9 (5.4) 17.3 (3.7) Amer. Indian/Alaska Nat., 756 48.3 (2.4) 16.5 (2.3) Education < HS 7093 23.4 (0.7) 23.7 (0.6) HS 14015 39.8 (0.6) 14.8 (0.4) > HS 33236 49.6 (0.4) 13.0 (0.2) Income (% of Poverty Level) < 100 6718 28.1 (0.9) 26.2 (0.7) 1-199 10678 32.4 (0.6) 18.8 (0.6) 2-299 8213 39.7 (0.8) 14.0 (0.6) 300 + 28735 51.8 (0.4) 11.1 (0.2) • Only about 50% of adult Californians meet the recommendation concerning moderate physical activity • Adherence to recommendations was more prevalent in males, Pacific Islanders, Non-Hispanic whites, the more educated, and those with higher incomes • Adherence differences decreased when non-leisure time walking and bicycling was added to leisure time physical activity, especially for race/ethnicity, education and income • These results highlight the importance of assessing physical activity in multiple domains, not just leisure time. Such efforts are especially important in economically and culturally diverse samples Methods 40 • Data from the 2001 California Health Interview Survey (CHIS: http://www.chis.ucla.edu/). • CHIS is a multi-purpose health survey conducted by the UCLA Center for Health Policy Research • CHIS 2001 included questions about leisure time physical activity as well as non-leisure time walking and bicycling • A statewide representative sample of > 50,000 US adults, conducted in multiple languages, with over-sampling of several ethnic groups • Data were analyzed with SAS and SUDAAN, incorporating sample weights and CHIS survey design characteristics. 20 0 >HS HS <HS Education 60 40 Definition of Adherence to Physical Activity Recommendation 20 Acknowledgements 0 150 min./week moderate activity, 60 min./week vigorous activity, or a combination totaling 150 minutes/week 300+ 2-300 1-200 <100 David Berrigan gratefully acknowledges the Cancer Prevention Fellowship Program of the National Cancer Institute for support while some of the work was performed Income (% of Poverty)








![[PDF READ ONLINE] The Spanish Workbook for Kids: A Fun and Easy Beginner's Guide to Learning](https://cdn7.slideserve.com/12419098/slide1-dt.jpg)