Download
1 / 50
650 likes | 1.32k Views
Acute Radiation Syndrome (A Spectrum of Disease). Doran Christensen, DO Associate Director, REAC/TS. Acute Radiation Syndrome. Systemic Effects from Acute Radiation Exposure Multi-Faceted Spectrum of Disease Involvement of One or more Organ Systems. Ionization Process .

E N D
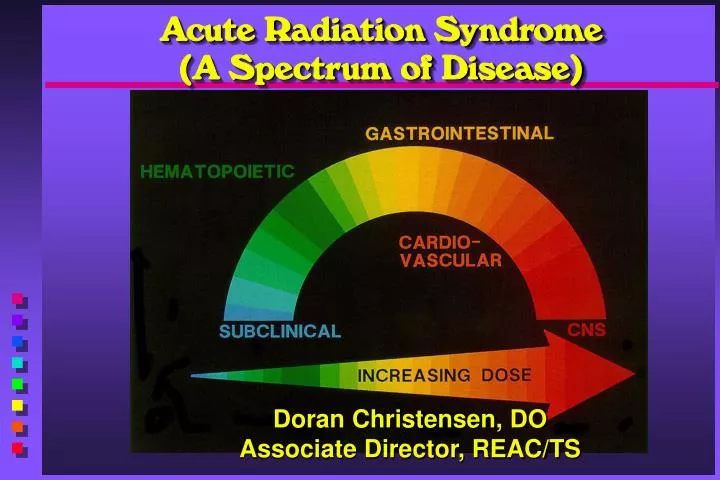
Acute Radiation Syndrome (A Spectrum of Disease) Doran Christensen, DO Associate Director, REAC/TS
Acute Radiation Syndrome • Systemic Effects from Acute Radiation Exposure • Multi-Faceted Spectrum of Disease • Involvement of One or more Organ Systems
Ionization Process • Density of Ionization Trail • Chemical Bonds • DNA Damage • Subcellular components • Mitotic Delay • Repair • Complete • Incomplete • Residual Damage? Measureable?
Exposure Principles • Total vs. Partial Body Irradiation • Threshold Effect of Dose • Threshold • D50 Dose • Dose Rate • Dose Protraction or Fractionation
Radiation Effects • Stochastic - “All-or-Nothing” Effect Occurrence Probability is Function of Dose • Increased Risk of Developing Cancer • Inheritable Mutations • Deterministic - Effect Severity is a Function of Dose (Commonly Associated with Threshold) • Inflammatory Response • Organ Failure • Fibrosis
Deterministic Stochastic 1 1 E E 0.8 0.8 f f 0.6 0.6 f f e e 0.4 0.4 c c 0.2 0.2 t t 0 0 Dose Dose Radiation Effects
Law of Bergonié and Tribondeau (1906) • More Differentiated Cells are Less Sensitive • Actively Proliferating Cells are More Sensitive • Radiosensitivity is Proportional to Mitotic and Developmental Activity Duration Rapidly Dividing Cells that Are Poorly Differentiated and Have a Long Mitotic Period Are Very Radiosensitive
Exceptions: • Lymphocyte - Most Radiosensitive Cell • Oocyte - Non Mitotic Cell
Radiosensitive Cells • Red Marrow • Epithelial Cells of GI System, Lung • Epithelium of Lens • Germinative Cells of Testis and Ovary • Endothelial Cells of Blood Vessels
Radiosensitive Cells (cont’d) • Pluripotential Stem Cells • Rapid Mitotic Rate • Form Intermdiate Precursors and then Mature Elements. • Cells with Large Nuclei • Interphase Death • Lymphocyte, Oocyte and Salivary Gland
Effects of Radiation Protraction Prodromal Component (Gy) Vomiting Diarrhea Brief Protracted Brief Protracted Exposure Exposure Exposure Exposure D50 2 5 3 6 Threshold 0.5 1.5 1 2.5 NUREG / CR 4214, Part II, p. 21
GI Cellular Hierarchy IAEA – UNSCEAR 1988
Skin Cellular Hierarchy IAEA – UNSCEAR 1988
Exposure Prodromal Stage Latent Stage Manifest Illness Recovery Time (60 days) Phases of Acute Radiation Syndrome
Acute Radiation Syndrome • Components of Radiation Effects: • Prodromal (0.5 - 3 Gy) • Hematological (1.5 - 6 Gy) • Respiratory (5 - 310 Gy) • Cutaneous (5 - 10 Gy) • Gastrointestinal (8 - 15 Gy) • Neurovascular (6 - 50 Gy) • Combined Injury
Prodromal Component(0.5 - 3 Gy and higher) • Immediate Effect of Cell Membrane Damage • Mediated by Inflammatory Elements of Cell Destruction • Mediated Neurologically by Parasympathetic System
TBI Dose Estimates for Prodromal Symptoms Prodromal Component (Gy) Vomiting Diarrhea Brief Protracted Brief Protracted Exposure Exposure Exposure Exposure D50 2 5 3 6 Threshold 0.5 1.5 1 2.5 NUREG / CR 4214, Part II, p. 21
Hematopoietic Component(1.5 - 6 Gy and higher) • Lymphocytes • Neutrophils • Thrombocytes • Erythrocytes
Hemogram3 Gy (300 Rad) TBI Exposure Source – REAC / TS Diagram – Human Irradiation 3 Gy (300 Rads)
Gastrointestinal Component(8 - 15 Gy and higher) • Symptoms • Mechanisms • GI Epithelial Sterilization - 15 Gy • Veno-Occlusive Disease of Liver
Respiratory Component(5 - 310 Gy and higher) • Sensitive from Highly Vascular Tissue • Endothelial Cells • Type II Alveolar Cell • Effect is Dose-Rate Related • Pneumonitis • Fibrosis
Pulmonary Lethality Syndrome Dose Rate (Gy/hr) Threshold (Gy) • 0.05 310 • 0.1 160 • 0.5 40 • 1 20 • 10 7 • 100 5 NUREG / CR-4214, Part II, p. 55
Neurovascular Component(8 - 50 Gy and higher) • Brain Cells are Fixed, Post-Mitotic Cells • Weak Link -- Stromal Cells • Endothelial Cells Turnover • 2 Months to 3 Years (3 Days) • EEG Changes Doses as Low as 1 Gy
Neurovascular Component (continued) • 1 - 6 Gy - Glial Cell Damage • 10 Gy - Morphologic Changes • 10 - 20 Gy - Vascular Lesions • 40 Gy - White Matter Necrosis • 60 Gy - Demyelinization
Ovarian Function Ovarian Dose (Gy) Results 0.6 - No Deleterious Effect 1.5 - Some Risk for Ovulatory Suppression in Women over 40 2.5 - 5.0 - 60% Women Aged 15-40 Have Permanent Suppression Remainder have Temporary Amennorrhea 100% Women Over 40 have Permanent Suppression 5.0 - 8.0 - 60-70% Women Aged 15-40 Have Permanent Suppression Remainder have Temporary Amennorrhea >8.0 - 100% Permanent Ovulatory Suppression NUREG / CR-4214, p II-70
Sperm Production Testicular Dose (Gy) Results 0.1 - 0.3 - Temporary Oligospermia 0.3 - 0.5 - 100% Temporary Aspermia from 4 - 12 mo Post-Irradiation Full Recovery by 48 mo 0.5 - 1.0 - 100% Temporary Aspermia from 3 - 17 mo Full Recovery Beginning at 8 - 38 mo 1 - 2 - 100% Temporary Aspermia from 2 - 15 mo Recovery Beginning at 11 - 20 mo 2 - 3 - 100% Aspermia Beginning at 1 - 2 mo No Recovery Observed after 40 mo NUREG / CR-4214, p II-73
Radiation Skin Injury • Effects • Time Frame • Injury Course
Radiation Skin Injury • .75 Gy - Hair Follicles Change • 3 Gy - Epilation • 6 Gy - Erythema • 10 Gy - Dry Desquamation • 20 Gy - Wet Desquamation (Transepithelial Injury)
Skin Effects Effect Parameter Brief Protracted Exposure Exposure Erythema Threshold 3 6 D50 6 20 Transepithelial Threshold 10 40 Injury D50 20 80 NUREG / CR-4214, p II-68
Skin Effects Effect Single Onset Dose (Gy) Time Epilation 3 - 7 ~18 days Erythema 10 - 20 12 - 17 days Pigmentation 10 - 20 Dry Desquamation 10 - 20 30 - 70 days Moist Desquamation 20 - 24 30 - 50 days That Heals Telangiectasia 17 - 24 6 mo - years Nonhealing Necrosis > 60 months, years NUREG / CR-4214, p II-68
El Salvador Patient + 32 Days Hyperpigmentation ( Bronzing )
El Salvador Patient + 32 Days Dry Desquamation
El Salvador Patient + 32 Days Transition to Wet Desquamation
El Salvador Patient + 32 Days Wet Desquamation
Triage • By Conventional Injuries • Trauma • Burns • By Radiation Injury • Prodromal Symptoms • Hematologic Picture
Modified USSR Classification (1986) • Class 1 Class 2 • Prodrome>3 hrs *1 - 3 hrs* • Lymphs (3-6 days)600 - 1000300 - 500 • TBI Dose1 - 2 Gy2 - 4 Gy • Survival EstimateProbable w / o txPossible w / o tx • Class 3 Class 4 • Prodrome.5 - 1 hr < .5 hr • Lymphs (3-6 days)100 - 200 <100 • TBI Dose4.2 - 6.3 Gy6 - 12, 16 Gy • Survival EstimateProbable w / txNot Likely Mettler FA, Kelsey CA, Ricks RC Eds. Medical Management of Radiation Accidents. Boca Raton: CRC Press, 1990, p. 72. *Barabanova A. REAC/TS Newsletter. Winter 1992, Oak Ridge, TN, p 1-2.
Andrews LymphocyteNomogram • Confirms suspected radiation exposure • Determines significant hematological involvement • Serial CBCs every 6 h From Andrews GA, Auxier JA, Lushbaugh CC: The Importance of Dosimetry to the Medical Management of Persons Exposed to High Levels of Radiation. In Personal Dosimetry for Radiation Accidents. Vienna, International Atomic Energy Agency, 1965, pp 3- 16
Goans Nomogram – The Next Advance Goans, RE, “Clinical Care of the Radiation-Accident Patient: Patient Presentation, Assessment, and Initial Diagnosis” in Ricks RC, Berger ME, O’Hara FM, The Medical Basis for Radiation Accident Preparedness – The Clinical Care of Victims, p18.
Combined-Injury Triage whenRadiation Doses are Known* Conventional Triage Changes in Expected Triage Category Categories if Injuries are following Only Trauma Whole-Body Radiation Dose (Gy) No Radiation Exists < 1.5 (150 rad) 1.5-4.5 (150-450 rad) > 4.5 (450 rad) Prodrome Onset < 3 h 1 – 3 h < 1 h Immediate Immediate Immediate Expectant Delayed Delayed Expectant Expectant Minimal Minimal Expectant Expectant Expectant Expectant Expectant Expectant *Decision based on whole-body radiation dose, assuming all casualties are wearing personal dosimeters Source: Medical Consequences of Nuclear Warfare, 1989, p. 39
Combined Injury -Total Body Irradiation + Burns Rat Model AFRRI Medical Effects of Nuclear Weapons Course “Triage and Treatnent of Radiation Casualties” Lecture, slide 35
Treatment Overview • Supportive Care • Surgical Recommendations • Selective Gut Decontamination • Bone Marrow Transplants (not as successful) • Biological Response Modifiers • Cytokines (more successful) • Complications of Acute Radiation Syndrome
Supportive Care • Fluid and Electrolyte Replacement • Reverse Isolation • Total Parenteral Nutrition • Empiric Antibiotics for Documented Infection
Supportive Care (cont’d) • Irradiated Blood Products • Enteral Feedings • Intravenous Glutamine • Sucralfate
Surgical Recommendations • Based on Immunocompetence Status (neutropenia immunocompetence) • Life-Saving / Major Surgery within 36 - 48 h • Elective Procedures until 45 - 60 days Following Hematopoietic Recovery Browne D, Weiss JF, MacVittie TJ, Pillai MV (eds) Treatment of Radiation Injuries, 1990, Plenum Press, New York, p. 229
Selective Gut Decontamination • Historical Background • Non-Systemic Abx vs. Systemic Abx • Fluoroquinolones • Ciprofloxacin, Ofloxacin • Norfloxacin
Cytokine Combinations • IL-3/G-CSF • IL-3/GM-CSF
Acute Radiation Syndrome Complications • Hematologic/Gastrointestinal • Interstitial Pulmonary Fibrosis • Veno-occlusive Disease of the Liver • Herpes Simplex (HSV) Reactivation • Cytomegalovirus (CMV) Reactivation • Combined Injuries
Any Questions? uncleofdisaster@cdc.gov
References • NUREG / CR-4214, Health Effects Models for Nuclear Power Plant • Accident Consequence Analysis: Low LET Radiation, Part II: Scientific Bases • for Health Effects Models, US Nuclear Regulatory Commission, 1989. • Browne D, Weiss JF, MacVittie TJ, Pillai MV (eds)Treatment of Radiation Injuries, • 1990, Plenum Press, New York, p. 229 • AFRRI Medical Effects of Nuclear Weapons Course “Triage and Treatnent of • Radiation Casualties” Lecture, slide 35 • IAEA, The Radiological Accident in San Salvador, 1989 • Ricks RC, Berger ME, O’Hara FM, The Medical Basis for Radiation-Accident • Preparedness – The Clinical Care of Victims, Parthenon Publishing Group, Inc: • New York:2002. • Saenger EL, Andrews GA, Linnemann RE, Wald N: Radiation Accident Preparedness • Medical and Managerial Aspects. Science-Thru-Media: New York 1981, p 15. Revision 6.1 – 17 Apr 2004