Download
1 / 35
410 likes | 1.02k Views
Cleft Lip & Palate. Eduardo D. Rosas Blum, MD August 7, 2007. While on call…. 25yo G1 P1 delivers a full-term infant after 12hrs of uneventful labor. The infant was found to have a cleft lip and palate. How should the care for this infant, and his mother, be?. Birth defects.

E N D
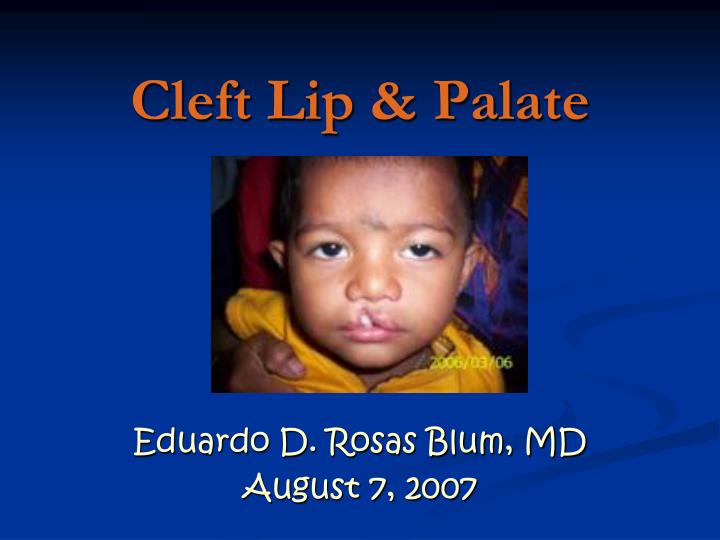
Cleft Lip & Palate Eduardo D. Rosas Blum, MD August 7, 2007
While on call… • 25yo G1 P1 delivers a full-term infant after 12hrs of uneventful labor. • The infant was found to have a cleft lip and palate. • How should the care for this infant, and his mother, be?
Birth defects • Malformations • alterations in normal development • Deformations • abnormal mechanical force on an otherwise normal fetus • Disruptions • disruption of an otherwise normal developmental process
Introduction • Most common craniofacial malformation • Cleft lip with or without cleft palate (CL/P) or isolated cleft palate (CP). • CL/P and CP differ with respect to • Embryology, etiology, candidate genes, associated abnormalities, and recurrence risk.
Prevalence • CL/P is more common than CP and varies by ethnicity. • CL/P • High in American Indians and Asians (1/500 newborns) • Low in American blacks (1/2000 newborns) • Intermediate level in Caucasians (1/1000 newborns) • Isolated CP occurs in only 1/2500 newborns and does not display variation by ethnicity.
Cleft Lip • Complete closure at 35 days postconception: • 7 weeks from the LMP. • Lateral nasal, median nasal, and maxillary mesodermal processes merge. • Failure of closure can produce unilateral, bilateral, or median lip clefting. • Left side unilateral cleft is the most common.
Cleft lip Severity • Mild, involving only the lip • Extend into the palate and midface thereby affecting the nose, forehead, eyes, and brain.
Cleft Palate • Lack of fusion of the palatal shelves. • Abnormalities in programmed cell death may contribute to lack of palatal fusion(?). • Isolated disruption of palate shelves can occur after closure of the lip • Palatal closure is not completed until 9 weeks post-conception.
Etiology Genes • Control cell patterning, cell proliferation, extracellular communication, and differentiation • Clefting usually represents a genetically complex event • Single Mendelian disorders associated with clefting are rare • 2 to 20 genes are thought to interact to result in facial clefting
Etiology • Dlx gene • Direct the destination of the distal skeletogenic mesenchyme elements to the palate. • Mutations of these genes result in isolated palatal defects. • Sonic hedgehog gene • Protein that mediates ectodermal functions, might regulate the outgrowth and fusion of the facial domains. • TGF-alpha variant • Receptor ligand, usually a rare variant of TGF-alpha • Family histories of cleft defects • Additive teratogenic effect with agents such as cigarette smoking and alcohol
Etiology • TGF-beta-3 gene • Expressed just prior to palatal fusion. • Results in isolated cleft palate. • IRF 6 • Identified in autosomal dominant van der Woude syndrome.
Environmental agents • Several agents that are associated with an increased frequency of midfacial malformation. • Medications —phenytoin, sodium valproate, methotrexate. • With corticosteroids there is no evidence of an increase in malformations. • Possible association could not be excluded
Etiology • Cigarette smoking • Noted with mothers of children with facial clefting, both CL/P and CP. • Teratogenesis has been attributed to hypoxia as well as a component of tobacco (cadmium). • Alcohol • Associated with an increased risk of fetal facial clefting. • Alterations in cell membrane fluidity or reduced activity of specific enzymes such as superoxide dismutase. • Folate deficiency • Contributes to a range of birth defects. • Evidence is emerging for a similar association with the development of CL/P.
Prenatal Diagnosis • Diagnosed until the soft tissues of the fetal face can be clearly visualized sonographically (13 to 14 weeks). • The majority of infants with cleft lip also have palatal involvement: • 85% of bilateral cleft lips • 70% associated with cleft palate. • Cleft palate with an intact lip comprises 27% of isolated CL/P
Prenatal Diagnosis • The sensitivity is highest when is associated with other structural anomalies. • Isolated CL/P in a low risk population, the sensitivity may only reach 50 percent. • Cleft palate with an intact lip is the most difficult orofacial malformation to diagnose prenatally. • Detected in only 13 of 198 cases in one large series. • Three-dimensional ultrasound, can provide a clear image of the malformation
Syndrome ? • A thorough examination of the newborn or stillbirth is always warranted. • Orofacial clefting is noted in over 300 syndromes. • 3 deserve additional comment. • frequency, variable presentations, and modes of inheritance
Deletion of chromosome 22q11 • DeGeorge syndrome. • Spectrum in addition to cleft palate: • Conotruncal cardiac defects, thymic hypoplasia, and velopharyngeal webs. • Majority of cases represent a new microdeletion • In families with conotruncal malformations and/or CP, further evaluation is appropriate.
Oral-facial-digital syndrome, type I • X-linked dominant syndromes. • Manifestations in affected females are variable and subtle: • hyperplastic frenula • cleft tongue • cleft lip/palate • digital anomalies
Treacher-Collins syndrome • Autosomal dominant disorder • Downward slanting palpebral fissures, micrognathia, dysplastic ears, and deafness. • Mental development is normal. • The mutations appear to increase cell death in the prefusion neural folds. • A family history with deafness, ear abnormalities, or CP.
Obstetrical Management • Amniocentesis for karyotype should be offered. • high rate of chromosomal defects • Difficulty in prenatal sonographic diagnosis supports chromosomal evaluation • As of January 2002, "in utero" correction had been attempted only once in Mexico • The child delivered prematurely and died at two months of life
Postnatal Management • The Care will entail attention, not only to surgical repair, but also more immediate needs such as feeding. • Primary lip repairs can often be undertaken at three months of age with palatal repairs around six months. • Additional surgeries as well as speech and orthodontic therapies are often needed. • The cleft Lip and Palate Association (www.clapa.com/) provides support and information for parents.
Cleft lip repair. The edges of the cleft between the lip and nose are cut (A and B). The bottom of the nostril is formed with suture (C). The upper part of the lip tissue is closed (D), and the stitches are extended down to close the opening entirely (E).
Feedings • Infants with CL/P have few feeding problems. • If the cleft involves the hard palate, the infant is usually not able to suck efficiently. • Experiment (special nipples or alternate feeding positions) • The infant should be held in a nearly sitting position during feeding • Prevents flowing to the back into the nose. • Should be burped frequently, (q 3-4min).
Feedings • It is important to keep the cleft clean • Breastfeeding is extremely challenging.
Haberman Feeder • Activated by tongue and gum pressure. • Milk cannot flow back. • Replenished continuously as the baby feeds. • Prevents the baby from being overwhelmed with milk. • A gentle pumping action to the body of the nipple will increase flow.
Family Care • Have a family meeting with both parents present. • Infant should be brought to the parents as soon the mother and the infant are in satisfactory condition. • Allow the parents to observe, react and ask questions about the infant. • Explained the defect and the how the surgeon will most likely correct the clefts. • Before and after pictures are helpful.
Family Care • Emphasize as possible to the parents the normal healthy features of the baby. • The baby should be present when the defect is explained, as ugly as the cleft might be. • Training the mother about feeding techniques and avoiding complications.
References • Klaus & Fanaroff. “Care of the high-risk neonate”. Saunders”. 5th edition. 2001 USA. • Colin D. Rudolph “Rudolph’s Pediatrics” McGraw-Hill. 21st edition. 2002. USA. • Christensen, K, et al. “Cleft-twin sets in Finland 1948-1987”. Cleft Palate Craniofac J 1996; 33:530. • Clementi, M, et al. “Evaluation of prenatal diagnosis of cleft lip with or without cleft palate and cleft palate by ultrasound: experience from 20 European registries”. EUROSCAN study group. Prenat Diagn 2000; 20:870. • Milerad, J, et al. “Associated malformations in infants with cleft lip andpalate: a prospective, population-based study”. Pediatrics 1997; 100:180. • Cockell, A, Lees, M. “Prenatal diagnosis and management of orofacial clefts”. Prenat Diagn 2000; 20:149.