Download
1 / 82
840 likes | 1.51k Views
NSTEMI and antithrombotics. Dr. Gilbert Boucher R4 Emergency Medicine McGill. Goals. Review definitions of Non-ST-elevation Myocardial infraction and related items. Prognostic factors. Current therapies. Special cases. What's New? .

E N D
NSTEMI and antithrombotics Dr. Gilbert Boucher R4 Emergency Medicine McGill
Goals • Review definitions of Non-ST-elevation Myocardial infraction and related items. • Prognostic factors. • Current therapies. • Special cases.
What's New? October 4 , 2001Practice Guidelines: Atherosclerotic Cardiovascular Disease September 1 , 2001Practice Guidelines: Atrial Fibrillation April 27 , 2001Practice Guidelines: Percutaneous Coronary Intervention April 27 , 2001Expert Consensus Document: Catheterization Laboratory Standard April 3 , 2001Consensus Conference Report: Care of the Patient with Adult Congenital Heart Disease April 2 , 2001Expert Consensus Document: Standards for Acquisition, Measurement and Reporting of Intravascular Ultrasound Studies March 1, 2001Teaching Slides: ACC/AHA Guidelines for the Management of Unstable Angina and Non-ST-Segment Elevation Myocardial Infarction January 1, 2001Consensus Conference Report: Mechanical Cardiac Support 2000: Current Applications and Future Trial Design November 1, 2000Clinical Competence Statement: Invasive Electrophysiology Studies, Catheter Ablation, and Cardioversion October 1, 2000Clinical Competence Statement: Stress Testing September 1, 2000Practice Guidelines: Management of Patients with Unstable Angina and Non-ST-Segment Elevation Myocardial Infarction September 1, 2000Consensus Conference Report: Myocardial Infarction Redefined—A Consensus Document of the Joint European Society of Cardiology/American College of Cardiology Committee for the Redefinition of Myocardial Infarction July 1, 2000Expert Consensus Document: Electron-Beam Computed Tomography for the Diagnosis and Prognosis of Coronary Artery Disease June 1, 2000 Training Statement: Adult Cardiovascular Medicine (COCATS) Revised 6/00 Task Force #5: Training in Nuclear Cardiology www.acc.org
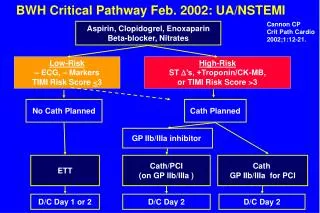
ACUTE CORONARY SYNDROME No ST Elevation ST Elevation NSTEMI NQMI QwMI Myocardial Infarction Unstable Angina
Myocardial infarction: acute, evolving, recent Typical rise and gradual fall (troponin) or more rapid rise and fall (CK-MB) of biochemical markers of myocardial necrosis with at least one of the following: • a) ischemic symptoms; • b) development of pathologic Q waves on the ECG; • c) ECG changes indicative of ischemia (ST segmentelevation or depression); or • d) coronary artery intervention (e.g., coronary angio-plasty).
Definition: NSTEMI ACC/AHA Guidelines • NSTEMI is an acute process of myocardial ischemia withsufficient severity and duration to result in myocardialnecrosis. • The initialECG in patients with NSTEMI does not show ST-segmentelevation. • NSTEMI is distinguished from UA by thedetection of cardiac markers indicative of myocardialnecrosis in NSTEMI and the absence of abnormalelevation of such biomarkers in patients with UA.
Definition: unstable angina • Unstable angina—an acute process of myocardial ischemiathat is not of sufficient severity and duration to resultin myocardial necrosis. • Donot release biomarkers indicative of myocardial necrosisinto the blood.
UA/NSTEMI3 PRESENTATIONS Rest Angina* Angina occurring at rest and prolonged, usually > 20 minutes New-onset Angina New-onset angina of at least CCS Class III severity Increasing Angina Previously diagnosed angina that hasbecome distinctly more frequent, longer in duration, or lower in threshold (i.e., increased by > 1 CCS)class to at least CCS Class III severity. * Pts with NSTEMI usually present with angina at rest. Braunwald Circulation 80:410; 1989
CAUSES OF UA/NSTEMI Mechanical Obstruction Thrombosis . Dynamic Obstruction MVO2 Inflammation/ Infection Mechanical Obstruction Thrombosis . Dynamic Obstruction MVO2 Braunwald, Circulation 98:2219, 1998 Inflammation/ Infection
The simplified criteria for Wellens' syndrome are as follows: Prior history of chest pain Little or no cardiac enzyme elevation No pathologic precordial Q waves Little or no ST-segment elevation No loss of precordial R waves Biphasic T waves in leads V2 and V3 or symmetric, often deeply inverted T waves in leads V2 and V3. Wellens' criteria are quite specific for left anterior descending artery disease. All of the patients (n=180) in his 1988 study had more than 50% narrowing of the left anterior descending artery (mean=85% narrowing) with complete or near-complete occlusion in 59%.
Troponins • I vs T… • Troponin I does not accumulate in renal failure • Different assays of same troponin have different values due to different isotopes of antibodies • Very sensitive • Estimate that 30% of patients with U/A are now diagnosed with NSTEMI due to elevated troponins • High correlation with death, being primary cardiac or not…
Figure 4 N Engl J Med 1996;335:1342–9.
Troponemia • Clin Chem 2000 46: 650-657. • 46 pts with septic shock • 36-50% had + trops • 12 pts nonsurvivors: negative autopsy for necrosis • Associated with severe LV dysfunction. • Clin Chem 2001 47: 412-417 • 244 pts, chronic hemodialysis, troponin T • Higher trops or increasing trops associated with death. • 6%, 43%, and 59% total death. • in 0%, 14%, and 24% cardiac death
Troponitis… • Clin Chem 1999:National Academy of Clinical Biochemistry Standards of Laboratory Practice: Recommendations for the Use of Cardiac Markers in Coronary Artery Diseases • Troponin I can be falsely elevated due to fibrin clot, heterophilic antibodies. • Use of 2 cut-offs point would require too much physician education… • AHA needs to better define NSTEMI due to important implication of being diagnosed with MI.
Figure 1. Plot of the appearance of cardiac markers in blood vs time after onset of symptoms. Peak A, early release of myoglobin or CK-MB isoforms after AMI; peak B, cardiac troponin after AMI; peak C, CK-MB after AMI; peak D, cardiac troponin after unstable angina. Data are plotted on a relative scale, where 1.0 is set at the AMI cutoff concentration.
Other markers • Delta values at 2 hours could proved to be very sensitive. • 2 hour delta CK-MB 88% sens vs delta trop I 61% • Specificity of 96% • ?early marker for more aggressive treatment AmJEmergMed - 2000 Jan • CRP: JACC 1998 Jun out of TIMI-11a • Neg trop but pos CRP = 5.8% death • Neg trop and neg CRP = 0.36% death • Pos trop and CRP = 9.1% death
Recommended • Class I: • Aspirin, Nitrate, B-blockers, morphine, O2 (prn). • Nondihydropyridine (cardizem/verapamil). • ACEi for specifics. • Class 2a: • ACEi for all. • Long-acting CCB for recurrent ischemia. • IABP if all fails. • Class 2b: • Extended form of Nondihydropyridine. • Short acting dihydropyridine in the presence of B-blocker.
Oxygen • For: • Cyanosis • Resp distress • High risk features • Consume resources • Evidence is lacking.
Nitrates: Decr MVO2, incr coronaries oxygenation Actions • Dilate venous bed: decr preload and ventricular wall tension. • Smaller dilatation of arterial system: decr afterload and ventricular wall tension. • Need B-blocker • Dilatation of atherosclerotic coronaries • Decreased platelets adhesiveness. • For • ischemia despite nitro X 3 and iv B-blockade • high-risk patients (non-hypotensive). • Prethrombolytics: 35% mortality reduction.
Morphine • Potent anxiolytic and analgesic action • Potentially beneficial • Venous dilatation • Decr HR • Decr sBP (Decr MVO2) • Activates neutral endopeptidases • Ann Emerg Med. May 2001;37:445-449. • Nausea and vomiting in 20% • Hypotension • Meperidine if allergic
Beta-blockers • Decr sBP • Decr SA node rate, contractility, AV node conduction. • Incr diastole filling time. • iv form for high-risk pts/on going pain. • Oral for intermediate/low risks patients. • No preferred agents except better if B-blocker without ISA (metoprolol, atenolol, propramolol, esmolol).
B-blockers • Contraindications (consensus): • 1st degre AV block >24 msec • 2nd or 3rd degre AV block without pacemaker • Asthma • Severe LV dysfunction with CHF • Caution with: • COPD • Bradycardia <50 • Hypotension <90 • Goal is bpm of 50-60 unless side-effects
B-blockers • 13% reduction of progression of UA to AMI. • Extrapolate data from use in AMI, recent MI, stable angina, heart failure.
Calcium channel blockers • Inhibit vasculature SM contracture • Coronary vasodilatation • Inhibit myocardial muscle contraction • AV block • Slow sinus node
Calcium channel blockers • Dihydropyridines: nifedipine and amlodipine • peripheral vasodilatation • Verapamil: DAVIT study (3200 pts) • Only favorable trend • Nifedipine: HINT study (500 pts) • Incr MI by 16%, decr by 20% if with metoprolol • But… metoprolol alone decr by 24%!!! • Diltiazem showed trends of improved outcome • CKMB level, reinfarction rate • Same mortality • … except in LV dysfunction ACS
Calcium channel blockers • Conclusion: • Good symptom reliever • Trend of improved outcome with non-dihydropyridine agents • To use if unable to use B-blockers
Antiplatelet agents • Aspirin ASAP! • Thienopyridine (clopidogrel or ticlopidine) if hypersensitivity of major GI intolerance
Aspirin • Cyclooxygenase-1 inhibitor • Prevents thromboxane A2 formation • Dosing: 160 mg or 325 mg • Based on ISIS-2 which definetly established its efficacy. • Can use pr route.
Adenosine diphosphate inhibitors • Clopidogrel acts faster than ticlopidine. • Ticlodipine: Gi se, neutropenia, TTP • Clopidogrel: minimal rash and diarrhea • 11 TTP within 14 days (3 millions pts) • CURE study: NEJM Aug 2001 • 12000 pts, plavix 300mg po • 9.3 vs 11.4, 16.5 vs 18.8 • ST changes or + markers • No GP2b3a inh or angio
Plavix:Safety if angio or used with Gp2b3A inh • Lancet August 2001: PCI-CURE study • 2600 pts. • Plavix 300mg loading • No increased bleeding problem whether plavix +/- GPIIb/IIIa inh were used. • Better outcome before an after PCI.
Other po agents • Sulfinpyrazone • Dipyridamole • Prostacyclin • Oral GP IIB/IIIA inhibitor: • 4 studies: 1 PCI, 3 NSTEMI • 2 increased mortality • None presently recommended
Anticoagulants • UFH • LMW heparin • Hirudin
UFH • Activates antithrombin III • Inactives thrombin (f2), f9a and f10a • Molecular weight: 5 000 to 30 000 D • Binds to various proteins, cells , endothelium • Unpredictable. • Weight adjusted dosage • Incr need in DM and smoking, lower with age • Theroux et al. N Engl J Med 1988;319:1105–11. • MI rate of 12% down to 0.8% in UA
LMW heparin • Molecular weight of 4200 to 6000 D • Factor Xa to thrombin inhibition ratio of 1.9 to 3.8 • Only 25-50% have >18 saccharides • both f2 and 10 inhibition • Rest inhibits only factor Xa
Figure 9 LMW heparin: ? better
Also… • Can only reverse about 60% of anticoagulation with protamine • Increase rate of minor bleeding (9.1% vs 2.5%) • Cannot monitor ACT during PCI, needs to stop 12 hours pre CABG. • Not for renal failure patients (GFR<30cc/min) • Decreased incidence of HIT. • >100kg: ?maximum of dosing vs study dosing • Enoxaparin 100mg sc bid vs weight all the way as in TIMI 11B
But going to cath lab… • Start UFH without bolus 6 hours after last dose. • If go to cath lab, consider pt fully anticoagulated when giving heparin boluses – unable to monitor. • If on UFH, wait 1 hour then give LMW heparin dose.
Hirudin • Direct thrombin inhibtor. • For patients with HIT or history of. • Binds directly to catalytic site of thrombin without going through antithrombin III • TIMI 7: better than ASA alone in UA… • Mild improvement compared to UFH but increase in bleeding, no benefit in STEMI. • Meta-analysis shows OR of 0.90
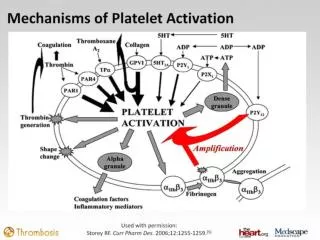
Platelet GP IIb/IIIa Receptor Antagonists • Activation of platelets leads to configurational change increasing affinity for fibrin and other ligands • Necessary final step to platelets aggregation. • Needs 80% blockade to achieve potent antithrombotic effects
GP IIb/IIIa Receptor Antagonists. • Abciximab (reopro): non-specific binding • Unclear significance • Eptifibatide (integrilin), tirofiban (aggrastat): very specific binding achieve >80% within 5 minutes • Different antagonists can bind at different sites and can paradoxically activates the GPIIb/IIIa receptor • ?what is happening with the oral form.
GP IIb/IIIa Receptor Antagonists • 4 main studies • 2 positives • High-risk features • 11.7% vs 8.7%, • 15.7% vs 14.2%