Download
1 / 15
160 likes | 296 Views
Repositioning Prevention and Control of Cancers of Reproductive Organs in Kenya. Dr. Gathari Ndirangu Ob/Gyn RH Technical Advisor. Cervix, Breast and Prostate. Equipment for screening and Rx Capacity building Advocacy Resources and support Resource mobilization including PPP

E N D
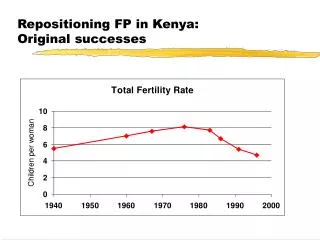
Repositioning Prevention and Control of Cancers of Reproductive Organs in Kenya Dr. Gathari Ndirangu Ob/Gyn RH Technical Advisor
Cervix, Breast and Prostate Equipment for screening and Rx Capacity building Advocacy Resources and support Resource mobilization including PPP Developments in routine HPV vaccination National Cancer Prevention and Control Bill, 2011
M&E • Data reporting tools • Incorporate indicators into HMIS • Integrated prevention, screening and Rx services • Male involvement • Community mobilization and community health strategy • Prevention, screening, early diagnosis and Rx • Palliative care
Cervical Cancer Prevention and Control in Women with HIV in Kenya
HPV-HIV Co-infection • Higher prevalence of persistent HR HPV infection • Higher prevalence multiple HR HPV types • Faster progression to CIN3 and ICC • 10y earlier • More advanced disease • Poorer histological types • Poorer prognosis • Effect of cART on ICC De Vuyst H, Lillo F, Broutet N, Smith JS (2008). HIV, HPV, and cervical neoplasia and cancer in the era of HAART. Eur J Cancer Prev 2008;17:545–54 Gichangi PB, Bwayo J, Estambale B, et al (2003). Impact of HIV infection on invasive cervical cancer in Kenyan women. AIDS 2003;17:1963–8.
HPV Vaccines in HIV-infected • HPV type distribution in HIV+ women similar to HIV- women* • HPV2 and HPV4 vaccines in WHIV • Similar immunogenicity between HIV- and HIV+ • * De Vuyst H, Ndirangu G, Moodley M et al. (2011) Prevalence of HPV in women with ICC by HIV status in Kenya and South Africa. Int. J. Cancer. DOI: 10.1002/ijc.26470
OR for multiple HPV infection in HIV+ versus HIV- women with cervical SCC, and by CD4 count and cART Higher Risk of Infection with Multiple HR HPV Types De Vuyst H, Ndirangu G, Moodley M et al., (2011) Prevalence of HPV in women with ICC by HIV status in Kenya and South Africa. Int. J. Cancer. DOI: 10.1002/ijc.26470
Screening in WHIV • Higher prevalence of benign cervical lesions e.g. ectopy, cervicitis • Lower VIA specificity (higher false-positive rates) • Over-treatment using the ‘screen and treat’ approach • Unnecessary exposure to side effects of CryoRx • Possible increased HIV shedding • Screen all WHIV in reproductive age • At HIV diagnosis • 6 months after diagnosis • Annually thereafter if the screening test normal
Management of CIN1 in WHIV • CIN 1 in WHIV has • High recurrence rates • Higher prevalence of HPV • More rapid progression to CIN 2/3 • Increased incidence of ICC • Rx of CIN1 does not reduce risk of progression • <50% clearance rates post treatment • No difference between LEEP and CryoRx • Close follow up is mandatory
Progression of cervical carcinogenesis Mild cytological abnormalities and/or CIN1 Precancer Cervical cancer Normal cervix HPV- infected cervix Persistent infection Infection Clearance: (approximate likelihood) CIN1: 57% CIN2: 43% CIN3: 32% Months Years > 20 years Progression CIN = cervical intraepithelial neoplasia.Precancer is equivalent to CIN2/3. Adapted from Schiffman M & Kruger Kjaer S. J Natl Cancer Inst Monogr 2003; 31:14–19.
Management of CIN 2/3 • Less successful than in HIV- women • High recurrence rates after Rx • Rx reduces risk of progression to ICC • Closer follow up
Post treatment Encourage • Adherence to cART • Prevention of re-infection • Male circumcision • Cessation of smoking • Expand integrated HTC and cervical cancer screening services
HPV Vaccines: In the Horizon • Second generation HPV vaccines • Additional HPV types • HPV9 (studies ongoing) • Incorporation of additional vaccine preventable diseases e.g. HSV? • Therapeutic vaccines • Thermostable vaccines • Mucosal surface vaccines? • Injection-free • Fewer doses? • Childhood administration? • Lifetime protection? • More affordable vaccines? • GAVI • Possible production in India?
Call for Action • Appreciate and recognize efforts by GOK • Continued advocacy • Leaders • Community • HRH and equipment • Conduct, share and disseminate research on cancer for policy formulation • Agents to reduce stigma • Palliative care