Download
1 / 48
580 likes | 1k Views
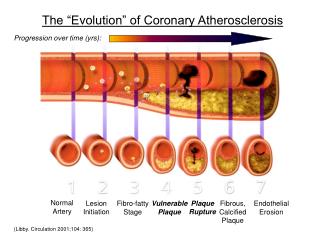
Pathophysiology of the coronary circulation : role of FFR. Giuseppe Biondi Zoccai University of Modena and Reggio Emilia, Modena, Italy gbiondizoccai@gmail.com. Functional significance of coronary stenosis. Past, present, future Pathophysiology Definitions and basics Other aspects.

E N D
Pathophysiology of the coronary circulation: role of FFR Giuseppe Biondi Zoccai University of Modena and Reggio Emilia, Modena, Italy gbiondizoccai@gmail.com
Functionalsignificance of coronary stenosis • Past, present, future • Pathophysiology • Definitions and basics • Other aspects
Functionalsignificance of coronary stenosis • Past, present, future • Pathophysiology • Definitions and basics • Other aspects
Basic coronary physiology •Coronary blood flow = 3-5% of CO •Resting myocardial O2 demand is extremely high(20 x skeletal O2 demand) •Myocardium extracts maximum O2 from blood (80% versus 30-40% skeletal muscle) •Myocardium has high capillary density (3000-4000/mm2 versus 500-2000/mm2 skeletal muscle) •Therefore, only way to meet increasing demand is to increase blood flow
Coronary circulation Myocardial blood flow = coronary flow (Qs) + collateral flow (Qc)
Coronary circulation Pressure derived flow measurements Pressure (Pmean) Blood flow (Q) = Resistance (R)
Coronary circulation Resistance distribution in the coronary tree
50% Coronary blood flow vs % diameter stenosis: Autoregulation of resting flow 85% 0% 1.0 Rest CBF Ml/gm/min 0 50 80 % Stenosis
Functionalsignificance of coronary stenosis • Past, present, future • Pathophysiology • Definitions and basics • Key aspects
Whatis FFR? FFR is a ratio or % of two flows: Maximum hyperemic flow in the presence of a stenosis FFR = Normal maximum flow FFR represents the extent to wich maximal myocardial blood flow is limited by the presence of epicardial stenosis FFR is a segment by segment evaluation of the flow
Pressurederived flow measurements ( Pd – Pv ) Pd (Pd – Pv) Q R = = FFR = = Pa myo (Pa - Pv) QN (Pa - Pv) R • Because the myocardial vascular bed is maximally vasodilated its resistance is minimal and constant. • Because, generally, central venous pressure is close to 0 R = Myocardial resistance at maximum vasodilation Pa = Mean aortic pressure PV = Mean central venous pressure Pd = Hyperemic distal coronary pressure
Relative pressure and relative flow QS = Flow in stenotic vessel QN = Flow in normal vessel Pijls et al, Circulation 1993;87:1354-67
Rationale of FFR ΔP = 30 mm Hg in all 3 cases but Driving pressure over the myocardium (wich determines myocardial perfusion at maximum vasodilatation) varies from 25 to 70 mm Hg Hyperemic blood flow is not determined by ΔPbut by (Pd-Pv)/(Pa-Pv) = FFR myo
Adenosine 40 µg IC Adenosine 40 µg IC • Intermediate stenosis • Mild-to-moderate stenosis • Non flow limiting stenosis • Non significant stenosis • Gross irregularity • ... Angiographist’s glossary FFR = 90 / 93 = 0.97 FFR = 50 / 92 = 0.53 Intermediate lesions 54-y-o. man, PTCA prox LAD 8 years ago, stable angina, occluded distal LCx 48-y-o. man, aborted sudden death, no other stenosis at angio
Coronary circulation Myocardial blood flow = coronary flow (Qs) + collateral flow (Qc)
An identical stenosis, but... • 26 col-schema fcf (figuur) 100 50 0 Pd Poor collaterals low FFR = 0.50
An identical stenosis, but... • 26 col-schema fcf (figuur) 100 75 0 Pd Good collaterals higher FFR = 0.75
Visiblecollaterals on the coronary angiogram (Rentrop) and fractionalcollateralblood flow Qc/Qn
Anatomicassesement of a stenosis Angiographicsignificance of coronary lesions % diameter stenosis 10 20 30 40 50 60 70 80 90 100 0 Discrete non-ischemic Critical Ischemic Severe Significant Ambiguous Borderline Intermediate Moderate Gould, Am J Cardiol 1974;33:87-94
Physiologic lesion assessment Threshold value of FFR to detect significant stenosis Gray zone FFR Non-signif. Significant stenosis 1.0 0.80 0.75 0 Sensitivity : 90% Specificity : 100% Pijls et al, New Engl J Med 1996; 334:1703-1708
Visualangiographicassessment vs FFR in the FAME trial Tonino et al, J Am Coll Cardiol 2010;55:2816-21
Functionalsignificance of coronary stenosis • Past, present, future • Pathophysiology • Definitions and basics • Other aspects
Acute microvascular damage in myocardial infarction STEMI Variable degree of reversible microvascular stunning Maximum achievable flow is less Smaller gradient and higher FFR across any given stenosis With time, the microvasculature may recover, maximum achievable flow may increase, and a larger gradient with a lower FFR may be measured across a given stenosis
Scar Normal Myocardium Similar stenosis but different extent of perfusion area 50 ml /min is too low Normal Myocardium 50 ml /min is sufficient FFR = degree of stenosis and extent of perfused miocardial mass
Hyperemic stimulants Jeremias et al, Am Heart J 2000;140:651-7
Hyperemic stimulants Casella et al, Am Heart J 2004;148:590-5
What about severe left ventricular hypertrophy? In severe left ventricular hypertrophy, there is an exaggerated increase of left ventricular mass in comparison to the vascular bed, resulting in the potential for ischemia even in normal or almost normal coronary arteries Thus, sensitivity may be reduced (cut-off >0.80?) However, specificity remains satisfactory
What about lesion length? Brosh et al, Am Heart J 2005;150:338-43
Take home messages • Normal value = 1.0 for every patient and every artery • FFR is not influenced by changing hemodynamic conditions(heart rate, blood pressure, contractility) • FFR specifically relates the influence of the epicardial stenosis toviable myocardial perfusion area and blood flow • FFR accounts for collaterals • FFR has a circumscriptthreshold value (~ 0.75 – 0.80 ) to indicate ischemia • FFR is easy to measure (success rate 99 %) and extremely reproducible • Pressure measurement has un unequaled spatial resolution(pressure pull-back curve) • Caution in acute myocardial infarction and LV hypertrophy
Thank you for your attentionFor any correspondence: gbiondizoccai@gmail.comFor these and further slides on these topics feel free to visit the metcardio.org website:http://www.metcardio.org/slides.html