Download
1 / 13
130 likes | 203 Views
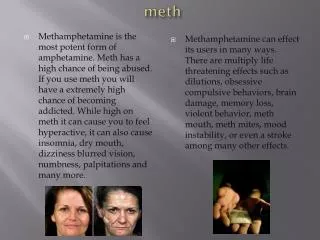
Efforts to Reduce Meth Use and Sexual Risk. Mary McFarlane, PhD Division of STD Prevention Centers for Disease Control and Prevention. Meth Withdrawal. Can last from 2-10 days Injectors suffer severe withdrawal Symptoms Depression Fatigue Anergia Paranoia Anxiety Agitation Confusion

E N D
Efforts to Reduce Meth Use and Sexual Risk Mary McFarlane, PhD Division of STD Prevention Centers for Disease Control and Prevention
Meth Withdrawal • Can last from 2-10 days • Injectors suffer severe withdrawal • Symptoms • Depression • Fatigue • Anergia • Paranoia • Anxiety • Agitation • Confusion Rawson (2006)
Challenges to success • Retention rates are low • Relapse rates are high • Severe paranoia and psychosis • Craving • Dysphoria • Anhedonia Rawson (2006)
Contrary to popular opinion… • Meth users respond to treatment in a similar manner as other substance abusers respond. • No differences between meth and other drug users in: • Retention rates • Urinalysis results during treatment • Treatment program completion rates Huber, Link and Rawson (1997)
Pharmacologic Treatment • No current medication effectively “treats” the withdrawal from meth or the craving • Some evidence indicates that these drugs may be helpful: • Bupropion • Methylphenidate SR Newton et al., 2005; Elkashef et al., 2006; Tiihonen,et al., 2006
Matrix Treatment Model • Elements of the model include: • Therapist support • Group/Individual participation • 12-step or other spiritual group involvement • Relapse prevention and education • Family involvement • Structure UCLA Integrated Substance Abuse Programs, 2006
Intervention Study for Methamphetamine-Dependent MSM • Treatment-seeking, meth-dependent MSM enrolled in behavioral intervention with 4 arms: • Gay-specific cognitive behavioral therapy (CBT) • CBT based on MATRIX • Contingency management (CM -- “peeing for dollars”) • CM + CBT • 40 participants in each arm Shoptaw et al, 2005
Research on Drug Treatment to Reduce Risk:Post-treatment Reduction of URA (30-day) Shoptaw et al., 2005
Results • The following behaviors significantly decreased for all conditions by 4 months post BL (end of treatments), and 6 and 12 month later: • recent meth use • recent URA • recent UIA • recent number of partners • No difference between groups Shoptaw et al, 2005
Sexual Risk Reduction Interventions for Substance Users: In Progress • Project MIX – DHAP, PRB (5-year project ending Sept 2007) • Meth-focused Intervention Pilot – DHAP, PRB (2-year project beginning Sept 2006)
Media Campaigns: Lack of Evaluation Data • Media approach to catch the attention of MSM and change norms, attitudes, and behaviors • Community mobilization around campaigns, but generally lack evaluation data • Examples from 2005: • “Huge Sale!” – HIV Prevention Forum, New York City • “Crystal Mess” – San Francisco DPH • Montana Meth Project (teens in general)
Summary • Treatment for meth dependence does exist and can be effective • Recovery is possible and many or most brain changes are reversed after abstinence • Is prevention of meth use possible?