Download
1 / 20
200 likes | 336 Views
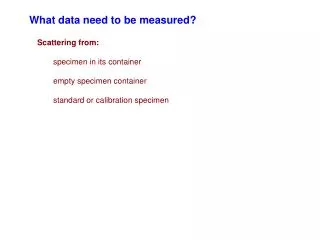
What does this specimen Show?. Optic Nerve Stained for Myelin. 7yr. male VP from Jamnagar. Left sided seizures – 2 episodes Referred for EEG from Jamnagar. Pt started on CBZ, not ready for MRI After 2 wks referred from opthalmologist for loss of vision, and optic neuritis

E N D
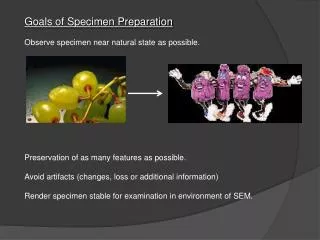
What does this specimen Show? • Optic Nerve Stained for Myelin.
7yr. male VP from Jamnagar • Left sided seizures – 2 episodes • Referred for EEG from Jamnagar. • Pt started on CBZ, not ready for MRI • After 2 wks referred from opthalmologist for loss of vision, and optic neuritis • MRI done- Diagnosis ADEM
ACUTE DISSEMINATED ENCEPHALOMYELITIS(ADEM) - A Clinical and Neuroradiological Profile of Pediatric Patients. Presented By Dr Jaimin M Patel M.D.(Paed) Under guidance of Dr.Varsha Tripathi M.D.(Paed),MRCP(London) Paediatric Neurologist With the help of Dr Manisha Shah. D. C. H.
Case History: ADEM • 4 year old male child • URTI for 3-4 days • Admitted with convulsions altered sensorium aphasia left hemiparesis • CSF prt: 72 mg/dL (40-60) cells: 8 cells/mm3 • MRI scan:(T2 weighted)asymmetrical hyper intensities in midbrain (more on right side) and middle cerebral peduncle suggestive of ADEM.
Case History: ADEM • Symptomatic treatment • IV methylprednisolone givenafter 48 hours no improvement- some deteriorationRt.third nerve palsybulbar weakness • IVIG given 1gm/kg/day for 2 daysRyles tube feeding started5 th day onwards improvement started child was hospitalized for 17 days • At present child completely normal, going to school
ADEM- Acute Disseminated Encephalomyelitis • Acute-Disseminated-Encephalo-Myelo-Itis (ADEM) • Usually monophasic • Demyelinating disorder • Characterized by diffuse neurologic signs and symptoms (polysymptomatic) • Nuroimaging- multifocal lesions of demyelination
Study… • Retrospective Study • Period : 14 months from Aug 2003 to Nov 2004 • Study Place: Medisurge and Sterling H. • Total No of Pts –13 • Mean Age – 4. 02 yrs. • M : F = 9 : 4
ADEM : Investigations • CSF (9 available) – 6 (66%) –normal, 3- (33%) Increase Pr. 1 (11%) -Pleocytosis • Mild mononuclear pleocytosis, raised proteins MBP content increased in 60% intrathecal oligoclonal immunoglobulins and IgG seen occasionally • CT Scan: (1 Pt-B/L hypodensities) (NOT INDICATED) • May be normal or may reveal areas of patchy low attenuation in the white matter.
MRI Scan R
ADEM : Investigations • MRI scan brain: • Multiple foci of demyelination in the cerebrum, midbrain, brain stem and cerebellum • Lesions are rather extensive and symmetric or asymmetric and more often located in the peripheral subcortical cerebral white matter. • Lesions in the thalami, hypothalamus and basal ganglia • Occasionally there can be cortical grey mater involvement also
ADEM: Treatment • High Dose Steroids • High dose IV Methyl Prednisolone 30 mg/kg/day for 3-5 days • followed by oral steroids (Prednisoslone)for 6 weeks • IVIG (<1 yr, No improvement in 48-72 hrs , AHLE, Recurrent) • 1 gm/kg/day iv for 2 days • Plasmapheresis • Symptomatic Rx
Relapse • Usually a monophasic illness • Multiphasic disseminated encephalomyelitis MDEM (Two in my study) • Recurrences : defined as appearance of new s/s at least 1 mth. after the previous episode. • 10-20% in different studies (2=15% in my study) • Recurrence appeared 1.5 - 32 months after initial presentation, but usually after steroids were stopped (2 months in my study) • 6 week taper shows less recurrences
PROGNOSIS • Complete recovery in 10 (77%) of the survivors • Relapsing disease in 2 (15%) • Mortality in 1 (7.6%) case. (Post Measles)