Download
1 / 27
320 likes | 714 Views
A 54-year-old man under GA, was found abnormal diaphragm movement during operation. Pneumothorax During Anesthesia. Presentation: Ri 周浩昌 / 林明恩 Supervisor: CR 黃信豪 VS 詹光政 Nov. 29, 2005. Brief History. 54 year-old man

E N D
A 54-year-old man under GA, was found abnormal diaphragm movement during operation Pneumothorax During Anesthesia Presentation: Ri 周浩昌/林明恩 Supervisor: CR 黃信豪 VS 詹光政 Nov. 29, 2005
Brief History • 54 year-old man • HBV carrier diagnosed by health check-up • Sonogram in 三重 hospital: - a small liver tumor(about 1*1 cm) • Abdominal CT in 亞東 hospital: - one tumor (1.6cm) at S#5-8 junctional area - and another tumor (1.2cm) at S#6 of liver suspected HCC
Past History • DM(-) HTN(-) • Alcohol consumption: social • Smoking: 1PPD for 40years and quit for 2 months • Allergy: NKA • Op history:Nil • Occupation: guard
Physical Examination • Vital signs: BP:122/78 mmHg, T/P/R: 36.8/76/18 • HEENT: Conjunctiva:pale, Sclera:anicteric • Neck: supple, LAP (-), JVE (-) • Chest: symmetric expansion, clear breathing sound • Heart: RHB, murmur(-)
Physical Examination • Abdomen: soft and flat, tenderness (-), rebound tenderness (-), shifting dullness (-), Liver/Spleen: impalpable; Bowel sound: normoactive • Back: CV angle knocking pain (-) • Ext.: edema(-), clubbing finger(-), tremor(-), petechiae(-), purpura(-), cyanosis(-)
Pre-OP assessment • A 54-year-old male • HBV carrier • Smoking: 1PPD for 40years and quit for 2 months • ASA class: II • Pre-OP CXR:
Operation: Segmental Hepatectomy 1. ETGA, supine position 2. Subcostal incision at right side, with xyphoid extension 3. Dissect abdominal wall in layers 4. Perform cholecystectomy 5. Mobilizationthe liver, echo for finding hepatic tumors 6. Segmental hepatectomy at S6 and S7 7. Check bleeding and close the wound in layers
Intra-operation(3) Abnormal diaphragm movement was found
Post-operation Condition(3) • 11/14 • 15:20- Demeral 40mg IV stat for pain • 15:30- CXR for 右胸微凸 • 15:40- Demeral 20mg IV stat for pain • 15:50- Pain relief, CXR showed pneumothorax • 16:40- Observation and keep O2 use - Keep SpO2 monitor
Post-operation Condition(4) • 11/16: • Mild decreased breathing sound over right side • Chest wall pain and sorethroat • No desaturation, mild dyspnea
Post-operation • Impression: Iatrogenic pneumothorax • Plan: Observation and supportive care • Discharged on 11/22 under stable condition
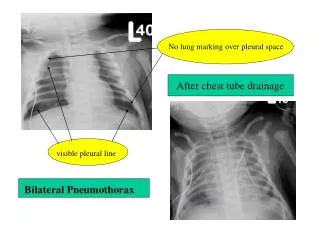
Discussion • Complication of CVC • Iatrogenic pneumothorax • Iatrogenic pneumothorax in anesthetized patient during operation • Tension pneumothorax in anesthetized patient during operation • Prevention
Diagnosis of Pneumothorax During Operation • General principles • Precipitating factors • Signs • Chest-X-ray • Needle test
Qual Saf Health Care 2005; 14: e18 General Principles • One of exclusion • Clinical observation: not reliable • Think of the possibility whenever the presence of high risk situations • Unilaterally decreased breathing sounds: • endotrachial intubation is most common • Tracheal deviation: • more likely due to slight rotation of head on • the neck
Qual Saf Health Care 2005; 14: e18 Precipitating Factors • Any needle or instrumentation, even days previously • External cardiac massage • Fractured ribs, crush injury • Blunt trauma/deceleration injury • Problem with pleural drain already sited • Airway overpressure, obstructed ETT • Emphysema or bullous lung disease
Qual Saf Health Care 2005; 14: e18 Signs • Increased PIP and decreased pulmonary compliance • Difficulty with ventilation/respiratory distress • Desaturation • Hypotension • Tachycardia • Unilateral chest expansion • Abdominal distension • Distended neck veins, raised CVP • Tracheal deviation
Qual Saf Health Care 2005; 14: e18 Urgent CXR • If there is any suspicion • May not detect a non-tension pneumothorax in a supine patient • Inspiratory AP and lateral views are preferable • In our case…
Qual Saf Health Care 2005; 14: e18 Needle Test • Needle aspiration of the pleural space or insert a short intravenous cannula • Needle test negative in deteriorating patient: • Loculated tension pneumothorax • Cardiac tamponade • 10 or 20ml syringe containing 3ml of water or • saline and 23G needle • Insert in: • - 2nd intercostal space, midclavicular line • - 4th intercostal space, midaxillary line • Small stream of bubbles: negative • Large bubbles: positive
Management of Pneumothorax During Operation Respiratory 2004; 9: 157-164
Qual Saf Health Care 2005; 14: e18 Management of Pneumothorax During Operation • Continuously observe the bottle for bubbling and/or swinging • Be vigilant for further deterioration in the patient • Increased or continuing air leak • Kinked/blocked/capped/clamped underwater seal drain • Contralateral pneumothorax • Misplaced pleural drain tip • Trauma caused by drain insertion • Misconnection of drain apparatus
Qual Saf Health Care 2005; 14: e18 Management of Pneumothorax During Operation • If the problem persists…. • Consider cardiac tamponade • - pericardiocentesis • - opening the chest
Tension Pneumothorax • In ventilated patients: - From simple pneumothorax when diagnosis is delayed - mortality rate in one previous study: 31% (Thorac Cardiovasc Surg 1974;67,17-23) - more serious in ventilated patients reaching 91% mortality rates in one series(Chest 2002;122:678–83 ) Emerg Med J 2005; 22:8-16
Tension Pneumothorax • The most common etiologies are either iatrogenic or related to trauma • Trauma (blunt or penetrating) • Barotrauma due to positive-pressure ventilation • Central venous catheter placement • Conversion of idiop athic, spontaneous, simple • pneumothorax Emerg Med J 2005; 22:8-16
Diagnosis of Tension Pneumothorax • Usually herald by a sudden deterioration in the cardiopulmonary status of the patient • Symptoms and signs • Clinical situation and the physical findings usually strongly suggest the diagnosis • Volume type ventilation • – peak pressure increase markedly • Pressure-support ventilation • – tidal volume decrease markedly • With Swan-Ganz catheters • – increased pulmonary artery pressures • –decreased cardiac output or cardiac index • Difficulty with ventilation / respiratory distress • Desaturation • Hypotension • Heart rate changes • Unilateral chest expansion • Abdominal distension • Distended neck veins, raised CVP • Tracheal deviation • Do not waste time trying to establish the diagnosis of • tension pneumothorax radiologically Murray and Nadel's Textbook of Respiratory Medicine, 4th edition
Murray and Nadel's Textbook of Respiratory Medicine, 4th edition Treatment of Tension Pneumothorax • High concentration of oxygen to alleviate hypoxia (Turn off N2O, FiO2 to 100%) • Support the circulation • Large-bore (14~16-gauge) IV catheter • Tube thoracostomy • Consider the possibility of bilateral pneumothoraces • Insert in: • - 2nd intercostal space, midclavicular line • - 4th intercostal space, midaxillary line • Diagnositic but may not completely relieve TPT
Delayed Pneumothorax Am J Emerg Med. 1995 Sep;13(5):532-5
Qual Saf Health Care 2005; 14: e18 Structural Thinking • SCARE • COVER ABCD - A SWIFT CHECK Circulation, Capnograph, and Color (saturation) Oxygen supply and Oxygen analyser Ventilation (intubated patient) and Vaporisers Endotracheal tube and Eliminate machine Review monitors and Review equipment Airway (with face or laryngeal mask) Breathing (with spontaneous ventilation) Circulation (in more detail than above) Drugs (consider all given or not given) A Be Aware of Air and Allergy SWIFT CHECK of patient, surgeon, process, and responses • Scan, check, alert/ready, emergency • - Scan: as needed, or every 5 minutes • - Check: whenever you are worried • - Alert/ready • - Emergency