Download

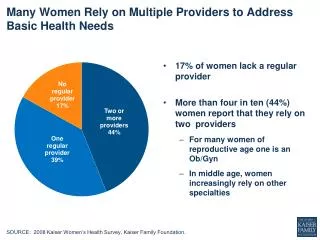
1 / 7
70 likes | 187 Views
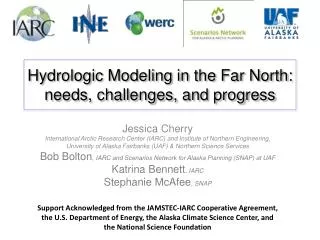
L inking A ctions for U nmet N eeds in C hildren ’ s H ealth. Examples of Implementation Strategies from Across the Country. Grantee Locations. Early Childhood Mental Health Consultation.

E N D
Linking Actions for Unmet Needs in Children’s Health Examples of Implementation Strategies from Across the Country
Early ChildhoodMental Health Consultation • DC-ECMHC meets w/child care providers weekly to increase staff capacity to recognize and support mental health. • MI-ECMHC works with foster families on using screening tools and strategies to enhance the foster caregiving experience. • IA-Creation of the Iowa Association for Infant and Early Childhood Mental Health will increase awareness of children’s mental health and promote professional development opportunities for the credentialing of ECMHCs.
Integration of Behavioral Health into Primary Care • RI-Development of Child Wellness Screen administered at 9, 18, 30 months and annually at age 3 years. Bilingual/bicultural AmeriCorps embedded in clinics assist families w/screenings. Clinician does follow up and referral. • OH-Interactive audiovisual media link between rural providers, families, and behavioral specialists. Consultation w/families occurs in primary care setting. Providers discuss and coordinate care for families. • MI-ECMHC outplaced in primary care offices for onsite consultation w/families and further evaluation if needed.
Screening and Assessment • WI-Coordinated state blueprint for implementing and funding developmental and S-E screening w/in primary care, ECE, child welfare, and EI. • TX-Training and ongoing support to providers on administration, interpretation, and follow up of ASQ:3, ASQ:SE, PEDS, and M-CHAT. Includes ToT and work with medical school residents. • CO-Using handheld devices as survey tablets. Patients can complete questions at home, waiting room, exam office and the interface allows a report to be printed immediately for the provider.
Parent Education andFamily Strengthening • CA-Preparing community organizations to implement Parent Café creating accessible and credible spaces for parents to meet, talk, and relect on their lives. • CT-Community-wide approach to the implementation of Circle of Security Parenting Program ensures year-round accessibility in five agencies. • NYC-Social-emotional development messages have been added to the pamphlet distributed with all birth certificates in NYC (12,000/month).
Home Visiting • ME-Bridging Program serves infants exposed to substances and their teen parents improves parent attachment by lowering stress and leveraging services that increase health outcomes. • MA-In-home cognitive behavioral therapy for mothers experiencing depression is an expansion of enhanced home visiting. • TX-Bilingual promotoras conduct home safety checks, developmental,depression, and substance abuse screenings and referrals, and use the Healthy Babies…Healthy Families curriculum