Download
1 / 66
751 likes | 1.04k Views
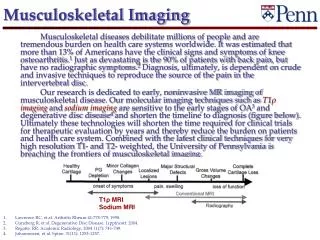
Introduction to Small Animal Musculoskeletal Imaging. Dr. LeeAnn Pack Diplomate ACVR. Musculoskeletal Radiography. Permit localization and characterization of a lesion Size, shape, margination, number, position, opacity Normal radiographic anatomy

E N D
Introduction to Small AnimalMusculoskeletal Imaging Dr. LeeAnn Pack Diplomate ACVR
Musculoskeletal Radiography • Permit localization and characterization of a lesion • Size, shape, margination, number, position, opacity • Normal radiographic anatomy • Diseases are often bilateral in the appendicular skeleton • Radiographic terms – use appropriately
Fractures:Principles of Radiographic Examination • 2 orthogonal views • Sedation/ anesthesia • Include joint above and below • Immediate post-operative repair radiographs should always be obtained • When needed, radiograph opposite limb for comparison (esp. in young animals)
Classification of Fractures • External communication • Open (compound) vs closed • Extent of damage • Complete vs incomplete • Direction and location of fracture line(s) • Simple, comminuted, multiple, etc….. • Stability • Location • Diaphysis, metaphysis, epiphysis • Special types => Salter-Harris, pathologic
Open (Compound) vs. Closed • Communicating wound to external surface open fracture • May see gas within soft tissues or large soft tissue defects • May see causal object (gunshot)
Extent of Damage • Complete => both cortices fractured • Incomplete => fracture through one cortex • Greenstick Complete
Direction and Location of Fracture Line • Simple => one fracture line • Transverse • Oblique • Spiral Transverse
Direction and Location of Fracture Line • Comminuted • Multiple fracture lines usually meet at a common point • One or more small fragments
Pathologic Fractures • Bone is weakened by pre-existing lesion • Fracture happens spontaneously • No history of trauma • Tumors, infection, hyperparathyroidism • Lysis may not be obvious • BIOPSY at the fracture site and do CHEST RADS if a fracture seems to have occurred for no reason!!!
Salter-Harris Classification of Physeal Fractures • Classification system developed by human physicians and adopted for animals • Correlated with prognosis • Higher number = higher chance of premature physeal closure (worse prognosis) • Premature closure • Bone foreshortening • Angular limb deformities
Salter-Harris Type I • Separation of metaphysis from epiphysis • Occurs through layer of hypertrophied cells
Salter Harris Type I Always do two views!!
Salter-Harris Type II • Most common • Fracture line travels through growth plate for variable distance then extends into metaphysis
Salter-Harris Type III • Fracture line travels through growth plate for variable distance then extends through epiphysis into articular surface
Salter-Harris Type IV • Metaphyseal fracture line extending through the physis and epiphysis to exit through the articular cartilage • Distal humeral condylar fractures
Salter-Harris Type V and VI • Type V – Compression of growth plate resulting from crushing force transmitted through physis • Type VI – eccentric physeal impaction resulting in transphyseal bridging
Radiographic Evaluation of Fracture Healing • ABCDs of fracture healing • Alignment of fracture segments • Bone healing and callus formation • Cartilage– implants away from joint, articular fxs • Device– appearance of implants (adjacent lysis, positional change) • Soft tissues– swelling, emphysema, atrophy
Radiographic Evaluation of Fracture Healing • The A’s • Apparatus • Alignment • Apposition • Activity
Fracture Healing Complications • Absence of callus formation • Instability/ large fracture gap • Zone of radiolucency around fixation devices • Bending or breaking of fixation devices • Fracture-associated sarcomas • Esp. femur (mean 5.8 yrs post-fracture) • Implant induced??
Implant Failure • Can see catastrophic failure with bending or breakage of implants • Lucency around implants • Loosening • Osteomyelitis
Nonunion Atrophic • When all signs of repair have ceased and further healing will not occur without surgical intervention • Types • Hypertrophic-”elephant’s foot” • Atrophic-sharp edges Hypertrophic
Malunion • A fracture that has healed in a position that is not anatomic
Soft Tissue Abnormalities • Intra-capsular soft tissues • Enlargement of soft tissue within the joint • Stifle, tarsus and carpus easiest to evaluate • Swelling usually conforms to joint margins • Can be caused by: • Effusion • Soft tissue proliferation • Tumor
Intra-capsular ST Swelling Normal IC Swelling
Bone Abnormalities • Bones response • Bone production - osteoblast • Periosteal reaction and sclerosis • Takes 12-14 days after insult • Bone loss – osteoclast • Lysis • 30-50% bone loss required to be seen on radiographs
Bone Loss • Determining Aggressiveness • Zone of transition • The less distinct the margin the more aggressive the lesion
Focal Bone Loss • Geographic Lysis • Large area of lysis • Usually less aggressive • If destroys the cortex aggressive
Focal Bone Loss • Geographic lysis • Expansile appearance • Expansion of the cortex around an enlarging mass less aggressive • Note the intact cortex in the picture
Focal Bone Loss • Moth Eaten lysis • Multiple smaller areas of lysis • Areas may become confluent • More aggressive than geographic lysis
Primary Bone Tumors • Radiographic Signs: • Lesion may be primarily productive, lytic or both • Lytic or productive lesions usually have an aggressive appearance • Away from the elbow and toward the knee
Primary Bone Tumors • Radiographic Signs: • Typically mono-ostotic • Typically located in the metaphysis • Lesions typically do not cross joints
Fungal Osteomyelitis • Radiographic Signs: • Typically lesions are seen in the metaphysis • Appear similar to primary bone tumor • Often extensive destruction when a joint is infected (septic arthritis) • Often is poly-ostotic
Fungal Osteomyelitis • Etiological Agents: • Blastomyces dermatitidis • Southern states, mid-west and south-west • Coccidioides immitis • Westernstates • Histoplasma capsulatum • Mid-western states • Cryptococcus neoformans & Aspergillosis • Throughout the US
Bacterial Osteomyelitis • Usually secondary to: • Gunshot wound • Penetrating wound ( dog or cat bite) • Previous surgery (implants) • Open fracture • May be seen secondary to septicemia in young animals or animals which are immuno-compromised
Bacterial Osteomyelitis • Radiographic Findings • Early = ST swelling • May take 10-14 days before periosteal reaction is seen • Periosteal reaction is typically solid and extends along the shaft of the diaphysis
Synovial Cell Sarcoma • Early in the disease there is intra-capsular and/or peri articular swelling • Swelling then turns to a mass effect • Later there is bone lysis of multiple bones of the joint
Cruciate Ligament Rupture • Cranial displacement of the infra-patellar fat pad • Caudal displacement of the fascial stripe
Cruciate Ligament Rupture • DJD • Base and apex of the patella • Proximal aspect of the trochlear ridge • Medial and lateral aspects of the distal femur and proximal tibia • Fabellae
OCD Shoulder Elbow Stifle Tarsus Retained Cartilage Core Fragmented Medial Coronoid Process Ununited Anconeal Process Panosteitis Hypertrophic Osteodystrophy Hip Dysplasia Legg-Calve-Perthes Developmental MS Diseases
Osteochondrosis • Subchondral defect – flattening • Surrounding sclerosis as time progresses • Joint mice • Secondary DJD • Locations: shoulder, elbow, stifle, tarsus
Shoulder OCD • Subchondral defect on the caudal aspect of the humeral head • May see a joint mouse • May just be flattened • Secondary DJD • May need arthrogram or explore