Download
1 / 35
350 likes | 520 Views
Applying NCQA PPC-PCMH Standards to Primary Care and Behavioral Health. Maria Ludwick, MPH Harold Pincus, MD. Agenda. PCASG Quality Improvement Program NCQA Patient Centered Medical Home Basics Adaptation to PC - BH Gaps in Implementation Strategies to Fill the Gap

E N D
Applying NCQA PPC-PCMH Standards to Primary Care and Behavioral Health Maria Ludwick, MPH Harold Pincus, MD
Agenda • PCASG Quality Improvement Program • NCQA Patient Centered Medical Home Basics • Adaptation to PC - BH • Gaps in Implementation • Strategies to Fill the Gap Note: This is a participatory session
Goals for the Primary Care Access and Stabilization Grant Increase access to care on a population basis Develop sustainable business entities Provide evidenced based, quality health care Develop an organized system of care
PCASG Quality Improvement Program • Interprets NoA requirement for a quality improvement program at the grantee level • Approved by CMS in June 2008 • Outlines a uniform set of quality standards • Minimum quality requirements • Optional incentive payment program • Encourages maximum participation • Based on National Committee for Quality Assurance (NCQA) Physician Practice Connections – Patient Centered Medical Home
Why NCQA PPC-PCMH? • Widely recognized for health care quality standards • Received input from a variety of stakeholders e.g. professional organizations, insurers, and patient advocacy groups • Standards emphasize use of systematic, patient-centered, coordinated care management processes • Reinforces partnerships between individual patients, and their personal physicians, and when appropriate, the family • Uses of registries, care coordination, information technology, and other means to assure patients have the right care when they need it • Standardized survey tool & methodology enables equitable distribution of PCASG funds • Encourages grantees to seek NCQA recognition
5% of PCASG grant funds available for QIP ($3.85M) 3 opportunities (March, June and Dec 09) ~$1.283M each payment Round One Awards Ranged from $67k-$135k Three Payment Tiers Based on NCQA levels but less stringent Graduated tiers/Graduated payments Half of an organization’s eligible service delivery sites must pass to obtain a specific tier Optional Quality Incentive Payment (QIP)
PPC-Patient Centered Medical Home Basics • Measures evaluate: • Use of systems • Effectiveness in prevention • Management of chronic illness and patient safety • Measures are “actionable” at practice level • Measures are validated by relating them to performance Score is based on: • Responses in Web-based Survey Tool • Supporting documentation attached to Survey Tool • Each element specifies type of documentation: Reports; Documented processes; Records or files
Data Sources & Guidance • Data sources and documentation are required • Each element indicate type of HIT required to perform functions • Basic – (HIT) Basic • Paper-based or administrative electronic system • Intermediate – (HIT) Intermediate • Electronic system for clinical functions • Advanced – (HIT) Advanced • Electronic system for connectivity or interoperability Practices can achieve a passing score on All Must Pass Elements with Basic Health Information Technology
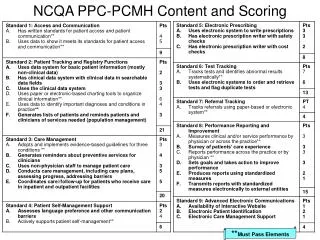
PPC-PCMH Content and Scoring **Must Pass Elements
NCQA PPC – PCMH Requirements: Must pass criteria 1A – Written standards for patient access 1B – Data to show it meets access standards 2D – Use charting tools to organize clinical info 2E – Data to identify 3 important conditions 3A – EBG for 3 conditions – 2 to pass 4B – Supports patient self management 6A – Test tracking 7A – Referral tracking 8A – Measure performance 8C – Report performance
Evidence-Based Chronic (Planned) Care Approaches for Treating Depression Are Effective Community Health System Resources and Policies Health Care Organization ClinicalInformationSystems Self-Management Support DeliverySystem Design Decision Support Productive Interactions Patient-Centered Coordinated Timely and Evidence- Efficient Based and Safe Informed, Empowered Patient and Family Prepared, Proactive Practice Team Improved Outcomes
Chronic Disease Clinical Models • Hypertension • Congestive heart failure (CHF)/Coronary artery disease (CAD) • Stroke • COPD (Chronic Obstructive Pulmonary Disease) • DM (Disease Management) • Asthma • Multiple comorbidities • Transitional care management
Depression Clinical Models • Chronic (planned) care model – Wagner • Collaborative care – Katon • Partners in Care (AHRQ) – Wells • PROSPECT – Alexopoulous, Katz, Reynolds • Telephone care management – Simon, Hunkeler • IMPACT (Hartford) – Unutzer • RESPECT (MacArthur) – Dietrich • Quality Improvement for Depression (NIMH) – Rost, Ford, Rubenstein • Child models – Campo, Asarnow, GLAD-PC • Other models for anxiety/PTSD
Leadership A Clinical Framework for Depression Treatment in Primary Care; Psychiatric Annals 32:9; September 2002
Delivery System Design A Clinical Framework for Depression Treatment in Primary Care; Psychiatric Annals 32:9; September 2002
Clinical Information System A Clinical Framework for Depression Treatment in Primary Care; Psychiatric Annals 32:9; September 2002
Decision Support A Clinical Framework for Depression Treatment in Primary Care; Psychiatric Annals 32:9; September 2002
Self-Management Support A Clinical Framework for Depression Treatment in Primary Care; Psychiatric Annals 32:9; September 2002
Functions of Care Managers A Clinical Framework for Depression Treatment in Primary Care; Psychiatric Annals 32:9; September 2002
Functions of Care Managers A Clinical Framework for Depression Treatment in Primary Care; Psychiatric Annals 32:9; September 2002
Phases of Depression Treatment Recovery Remission Relapse Recurrence No Depression Response Symptoms Syndrome Treatment Phases Acute Continuation Maintenance Kupfer DJ. J Clin Psychiatry. 52(5s):28-34,1991.
Top Ten Issues General Health/Mental Health Relationships • Partnerships • Formalize • Accountability • Referral • Consultation/Evaluation • Information Flow • Money • Quid Pro Quo • Maintenance • Generalize
Gaps (1) Participant comments NCQA Reports
RESULTS FROM Round One NCQA Surveyed Sites36 Sites Total 34 Primary Care 2 Behavioral Health
Where QIP Participants Did Well * PCASG Quality Minimum Requirement
Successes Reporting on Access & Communication Charting Tools Care Management Challenges Clinical Data System for Population Management Self Management Support Test Tracking Behavioral Health Organizations Challenges & Successes
Successes Processes for Access & Communications Charting Tools Challenges Reporting on Access & Communication Clinical Data Systems System for Population Management Care Management Continuity of Care Self Management Support Test Tracking Primary Care Organizations Challenges & Successes
Gaps (2) Organizing care management Tasks/Roles/People Incorporating self management Disease registries Referral tracking Communication/HIPAA Test tracking Guideline-based reminders Using data for QI Continuity of care Anticipation of needs
Care Management Functions Patient engagement/rapport Screening/Assessment Education/Planning Self management support Clinical monitoring/Tracking Reminders (patient/provider) Accessing resources/referrals Coordination/Continuity Problem solving/counseling/therapy
Top Ten Issues General Health/Mental Health Relationships • Partnerships • Formalize • Accountability • Referral • Consultation/Evaluation • Information Flow • Money • Quid Pro Quo • Maintenance • Generalize