Download
1 / 20
220 likes | 395 Views
Lower Back Pain . Dr Angela Jenkins ST3 Anaesthetics 10 th September 2008. Introduction. Epidemiology Presentation Investigations Management Conclusions. Epidemiology. Incidence - Lifetime prevalence 60-85% - Peak incidence age 40-60y - No difference between male and female

E N D
Lower Back Pain Dr Angela Jenkins ST3 Anaesthetics 10th September 2008
Introduction Epidemiology Presentation Investigations Management Conclusions
Epidemiology Incidence - Lifetime prevalence 60-85% - Peak incidence age 40-60y - No difference between male and female - More common in heavy, manual occupations - Increased incidence in smokers
Epidemiology • Impact on Society • Approx 52 million working days lost per annum • 500 000 people receive Incapacity Benefit • £481 million pa cost to NHS • £5 billion pa cost to society • 50% chance of returning to work after 6 months absence
Transition from Acute to Chronic Pain • Risk factors: • Signs of nerve root involvement • Ongoing compensation claim • Long time off work • Psychological distress +/- depression • Poor physical fitness • Heavy smoking
Presentation Simple musculoskeletal pain (95%) Spinal nerve root pain (4-5%) Serious spinal pathology (~1%)
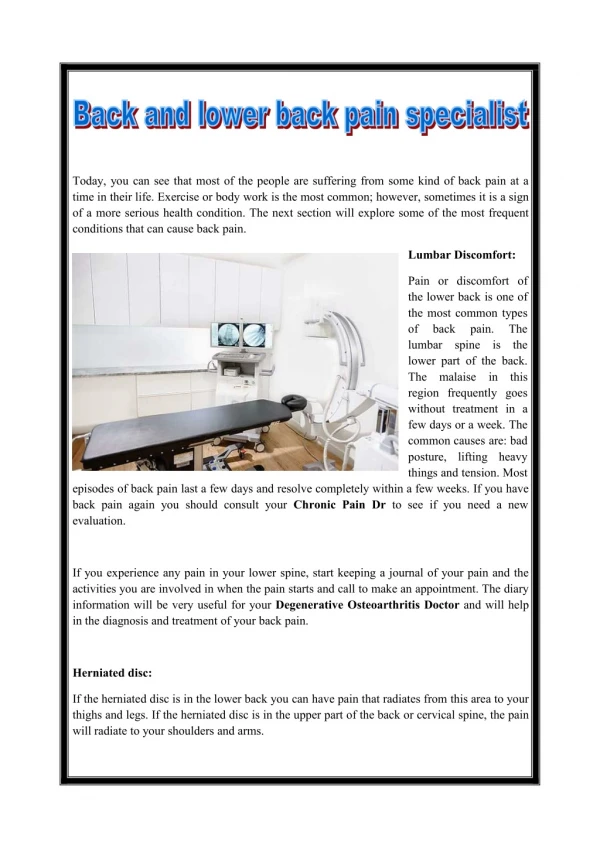
Musculoskeletal Back Pain Mechanical in nature Age 20 – 55 years Pain in lumbosacral area and buttocks Referred into upper thighs Dull ache, varies with activity Otherwise physically well
Musculoskeletal - Causes Discogenic pain Sacroiliac Joint pain Facet Joint pain Ligament and Muscle pain
Nerve Root Pain Well localised, sharp, electric shock-like Dermatomal radiation down leg into foot Neuropathic element worse than back pain May have paraesthesia +/- loss of reflexes Exacerbated by coughing, straining, sneezing Nerve root pain with SLR test
Nerve Root - Causes Posterior Disc Herniation Spinal Stenosis Epidural Adhesions
Serious Spinal Pathology • Differential Diagnosis • Spinal tumours / myeloma • Infection • Trauma • Inflammatory disease • Cauda Equina Syndrome • AAA • Retroperitoneal fibrosis
Serious Spinal Pathology • ‘Red flag markers’ • Age <20y or >55y • Constant / progressive pain • Acute onset in the elderly • H/O tumour • Fever / night sweats • Immunosuppression / HIV • Recent bacterial infection • Acute neurological symptoms • Unexplained weight loss • Systemically unwell
Serious Spinal Pathology • Examination • Tenderness on SI springing • Multiple nerve root signs • Dissociative signs • Symmetrical limitation of SLR • Signs of lower limb ischaemia • Abdominal mass
Investigations • Radiology • X-ray, CT, MRI, isotope bone scan • Blood tests • FBC, ESR, Ca, plasma viscosity • Nerve conduction studies • Diagnostic nerve blocks
Management • Aims: • Improve pain • Optimise physical, psychological and social functions
Management • Pharmaclogy • NSAIDs • Anti-depressants • Anti-convulsants • Opioids • Anti-spasmodics • Psychology • CBT • Pain management programmes
Management Physiotherapy TENS Accupuncture Injections Radiofrequency Lesioning Spinal Cord Stimulation Surgery
Conclusions Consequences may be more problematic than the pain itself Huge cost to society and NHS Multiple presentations / causes Must exclude serious pathology Multi-disciplinary management