Download
1 / 24
490 likes | 3.04k Views
ANION GAP . Dr. S. Parthasarathy MD ., DA., DNB, MD ( Acu ), Dip. Diab . DCA, Dip. Software statistics Ph d ( physio ) Mahatma gandhi medical college and research institute, puducherry , India . What is Normal ??. In serum , number of anions = number of cations

E N D
ANION GAP Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics Ph d (physio) Mahatma gandhi medical college and research institute, puducherry, India
Whatis Normal ?? • In serum, • number of anions = number of cations • (Na + K+ Ca2 + Mg2 + Protein) - ( Cl + HCO3+Protein +HPO4 +SO4) • Some are measurable but others are not • So comes the gap
Why unmeasured cations ?? • total unmeasured anions exceed the total unmeasured cations, there is an anion gap.
To calculate • Anion gap = (Na+ + K+ ) – ( HCO3- + Cl-) • (140 + 5) – ( 25 + 104 ) • 145 – 129 = 16 meq • Unmeasured anions • sulphates and a number of serum proteins.
Methodology of estimation • values were based on sodium concentration • determined by flame photometry, chloride concentration by a colorimetric method (usually mercuric-nitrate thiocyanate), • and total CO2 content by acidification of the specimen followed by colorimetric titration
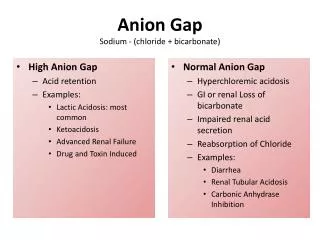
Anion gaps are important in acidosis • Anion gap can be classified as either high, normal or, in rare cases, low • High means what ?? • ([Na+] + [K+]) − ([Cl−] + [HCO3−]) • a loss in HCO3− without raise in Cl−
Increased anion gap acidosis • DKA. • Lactic acidosis • Alcohol intoxication • Salicylate poisoning • Azotemia • In all these, acidosis sets to deplete HCO3 but !!
Values • Normally 16 • Increased means around 22 • 45 are reported only one case of 90 is reported • Low means usually around 4
CUTE DIMPLES- pneumonic • Cyanide , • uremia • Toluene • Ethylene glycol • DKA • INH, • Methanol • Propylene • Ethylene glycol • Salicylate
Increased anion gap • Anion gap = (Na+ + K+ ) – ( HCO3- + Cl-) • There is no increase in Cl- • Gap widens • Usually above 22 meq
Diagnosis and severity of acidosis • ∆ AG is inversely proportional to ∆ HCO3 anion gap • HCO3 decrease anion gap increase • But latter this may not be there
Causes • Administration of chlorides • Carbonic anhydrase inhibitors • Pancreatic fistula • Ureterocolic fistula • Renal tubular acidosis
HCO3 decreases but Cl increasesi.e. the retention or excess of hydrochloric acid • Anion gap = (Na+ + K+ ) – ( HCO3- + Cl-)
FUSEDCARS - pneumonic - Causes • Administration of chlorides • Carbonic anhydrase inhibitors • Pancreatic fistula • Ureterocolic fistula • Renal tubular acidosis
Examples • Ammonium chloride ingestion • Diuretic • NH4 → NH3 + H+ ion • But chloride remains • Renal tubular acidosis – reabsorbtion of bicarbonate or excretion of hydrogen ions • Anions of metabolic acids like phosphates sulfates get excreted , Chloride increases • Hence anion gap is normal
RTA • loss of bicarbonate, along with its counterbalancing cation sodium, produces volume contraction, thereby stimulating the renal tubule to retain sodium chloride. • The consequences of these events are the replacement of sodium bicarbonate by sodium chloride.
Examples • Nacl administration (150 + 150) ↓ • NaHCO3 excreted ↓ retention of Hydrogen ions and chloride ions NAGMA
Gaps in anion gap • Decreased anion gap • Decreased unmeasured anions • Why ?? Range ! 1% • Hypoalbuminemia • Albumin decreased 4 to 3 gm ↓ anion gap 2.75 meq • Lab errors
Gaps in anion gap • Abnormal cations • Paraproteinemias • Lithium or bromine poisoning • Water excess • All electrolyte decreased by 10 % • (127 + 3) - ( 24 + 92 ) • 130 - 116 = 14
Gaps in anion gap • Serum chloride concentration was raised by approximately 3 mEq/L for every 1-mEq/L increase in the concentration of bromide • lithium is a cation, it can lower the serum anion gap when present in sufficient concentration • Hypercalcemia as a result of primary hyperparathyroidism, the serum anion gap was reduced by approximately 2.4 mEq/L
Anion gap – summary • Serum cations = anions • Anion gap = (Na+ + K+ ) – ( HCO3- + Cl-) • Unmeasured anions • HCO3 decrease is acidosis but sometimes Chloride increases to maintain anion gap in acidosis • There are some gaps