Download
1 / 73
2.03k likes | 4.76k Views
Humidified High Flow Oxygen Therapy. Clinical Application Ken Miller, MEd-RRT-NPS Educational/Research Coordinator Respiratory Care LVHN. Conflict of Interest.

E N D
Humidified High Flow Oxygen Therapy Clinical Application Ken Miller, MEd-RRT-NPS Educational/Research Coordinator Respiratory Care LVHN
Conflict of Interest I have no real or perceived conflict of interest that relates to this presentation. Any use of brand names is not in any way meant to be an endorsement of a specific product, but to merely illustrate a point of emphasis.
Objectives Learning objectives for this presentation: Describe the technological elements of High Flow Oxygen Delivery System. Define the clinical end-points when utilizing High Flow Oxygen Delivery System. Review outcome data and case scenarios with High Flow Oxygen utilization.
What is High FlowOxygen (HFO2) An oxygen delivery system which blends oxygen/air from 35%-100% Can be administered via wide bore nasal cannula or trach adapter up to 60 L/min. Provides humidity enriched oxygen therapy for patients in mild to moderate respiratory distress. HF02 does not augment tidal volume and thus does not facilitate CO2 removal. It is not a substitute for NIPPV in an acute crisis. However, it may provide a bridge from NIPPV to conventional oxygen delivery devices and also may give some patients NIPPV free hours.
High Flows Oxygen Benefits – There are five key benefits: Delivers a high FIO2 accurately Meets the patient’s ventilatory demands Provides patient comfort Provides a modest amount of positive airway pressure Optimizes mucociliary clearance
How is High Flow Oxygen Delivered? A combination of: Molecular high humidification delivery system An air/oxygen blender Flowmeter Via nasal cannula or trach tube adaptor
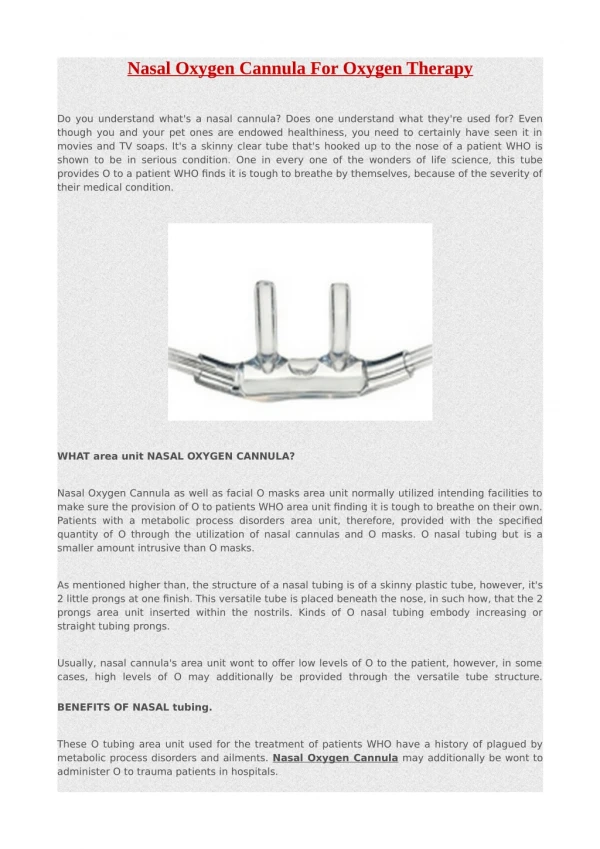
The prongs are wide bore dispersing the flow as it enters the nares and reduces the jetting effect associated with standard nasal cannula
Vent Tie-II Utilized for securing
Max Venturi Oxygen analyzer Allows for independent control of oxygen and flow FIO2 control Flow rate control
850 Humidifier provides molecular humidification Set a non-invasive mode via cannula
Complete High Flow Oxygen System set up
Were Does the Clinician Intervene with HFO2 in the Care Cycle? Invasive ventilation HF02 Non-invasive ventilation Face mask oxygen Humidity therapy HF02 Nasal cannula
High Flows of Oxygen Delivered Through Nasal Cannula The combination of nasal cannula and optimal humidity enables comfortable delivery of high flows Patient comfort Optimized patient outcomes Patient compliance
Why Improvement in Oxygenation? Guaranteed FI02 delivered Ventilatory demands met “Back pressure CPAP” -Every ten liters of flow approximately 1 cm of CPAP is generated! -Maximum of 5-6cm CPAP can be achieved.
Meeting patient’s inspiratory flow demand No ambient entrainment
Face-mask oxygen delivery vs High Flow Oxygen Approximately 1 cm/h20 of “back pressure CPAP” per every ten liters of flow
Where to Start High Flow Oxygen FI02 70% 40 lpm
SpO2 Monitoring A SpO2 monitor is to be utilized for ALL HFO2 patients and low SpO2 alarm must be set 2% below the physician ordered desired Sp02. The high respiratory rate alarm must also be set per physician order on the appropriate bedside monitor.
Weaning of HFO2 Titrate to 40% oxygen Reduce Flow to 20-30LPM Transition to nasal cannula
Outcomes • Sixty patients were placed on HFNC from July 1, 2009 to Dec 31, 2009 in MSICU. • In the HFNC that did not required therapy escalation had a 11.5 duration in MSICU compared to 19.5 who did.
Hypothesis • HFO may reduce escalation of therapy in specific patient populations that exhibit certain clinical and demographic characteristics
Relevance to Practice • Aid clinical decision making as to whether or not HFO is the best option for a specific patient • Initiate HFO on patients that display characteristics deemed successful • Not consider HFO for patients that display characteristics deemed unsuccessful • Effective and efficient use of respiratory technology
Study Design • Retrospective observational study • Analyzed data on patients at LVHN who were placed on HFO from May 21, 2011 to May 21, 2012 • Sample size: 137 patients • Patients less than 18-years-old were excluded • Patients on HFO were identified from a daily report received by respiratory therapy • Electronic medical record was used to gather demographic and clinical information regarding these patients
Methods • Patients were separated into two groups: patients who were successful on HFO and patients who were not • Success was defined as de-escalation in care, meaning the patient maintained clinical end-points on HFO or conventional oxygen delivery systems • Failure was defined as escalation in care, meaning that in order to maintain desired clinical end-points either NIPPV or mechanical ventilation had to be instituted • If a patient was on HFO for more than 72 hours they were counted as a failure because HFO is not indicated to be a long-term therapy1