Download
1 / 25

E N D
Cryptococcus neoformans Dr.T.V.Rao MD Dr.T.V.Rao MD
Cryptococcosis Chronic, subacute to acute pulmonary, systemic or meningitic disease, initiated by the inhalation of the fungus. Primary pulmonary infections have no diagnostic symptoms and are usually subclinical. On dissemination, the fungus usually shows a predilection for the central nervous system, however skin, bones and other visceral organs may also become involved. Distribution: World-wide. Aetiological Agent:Cryptococcus neoformans.
Cryptococcus neoformans • A Capsulated yeast – A true yeast.. • A sporadic disease in the past. • Most common infection in AIDS patients. Dr.T.V.Rao MD
A true yeast Round 4 – 10 microns Surrounded by Mucopolysaccharide capsule. Thick in vivo Negative staining with India Ink and Nigrosin 60% of the infected prove positive by India Ink preparation on examination of CSF KoH preparations in Sputum and other tissues, PAS and Mucicaramine staining helps confirmation. Morphology Dr.T.V.Rao MD
As Seen in India Ink preparation Dr.T.V.Rao MD
Culturing • CSF -Culturing on Sabouraud's agar, and incubated at 370 c for up to 3 weeks • Cultures appear as Creamy, white, yellow Brown colored Simple urease test helps in confirming the isolate. Dr.T.V.Rao MD
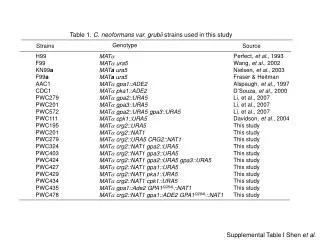
A true yeast 4 serotypes - A,B,C,D A and D - C.neofromans var neoformans B and C - C.neoformans var gatti. Many infections are caused by C.neofromans var neoformans. Found in wild/Domesticated birds. Pigeons carry C.neofromans, Birds do not get infected. Cryptococcus neoformansSerotypes Dr.T.V.Rao MD
Serotypes - Cryptococcus neoformans Serotype A – 80% clinical cases B – tropical, subtropical – S. California, Hawaii, Brazil, Australia, SE Asia C – rare D – Europe – Denmark, Germany, Italy, France, Switzerland
Pigeons and Red river gum tress harbors the Cryptococcus in nature Dr.T.V.Rao MD
Life cycle of C.neofromans Dr.T.V.Rao MD
Enters through lungs - inhalation of Basidiospores of C neoformans Enters deep into lungs, Men acquires more infections, and women less infected. Self limiting in most cases, Pulmonary infections can occur. Present as discrete nodules - Cryptococcoma. Pathogenesis Dr.T.V.Rao MD
Can infect normal humans Abnormalities of T lymphocyte function aggravates, the clinical manifestations. In AIDS 3- 20% develop Cryptococcosis. Present with Chronic meningitis , Meningo encephalitis Manifest with – head ache low grade fever, Visual abnormalities ,Coma – fatal Treatment reduces the morbidity and cure in non immune suppressed expected. Pathogenesis Dr.T.V.Rao MD
Can manifest with involvement of ,Skin, mucosa,organs,Bones,and as Disseminated form. Can mimic like Tuberculosis, Pathogenesis Dr.T.V.Rao MD
Lung - Portal of entry - asymptomatic (1/3) life threatening pneumonia (ARDS) Endobronchial colonization underlying chronic lung disease Single pulmonary nodule Symptomatic – acute, sub acute Clinical Manifestations
CNS Sub acute meningitis or meningo-encephalitis Headache, fever, cranial nerve palsies, lethargy, coma Subacute (days) months HIV Higher yeast burden incidence raised intracranial pressure Often disseminated Immune reconstitution disease Clinical Manifestations
CNS Subacute meningitis or meningo-encephalitis Headache, fever, cranial nerve palsies, lethargy, coma Subacute (days) months HIV Higher yeast burden incidence raised intracranial pressure Often disseminated Immune reconstitution disease Clinical Manifestations
CSF Microscopic observation under India Ink preparation Direct microscopy - Gram staining Cultures on Sabouraud dextrose agar, Serological tests for detection of Capsular antigen CSF findings mimic like Tuberculosis IN CSF - latex test for detection of Antigen Blood cultures, ELISA Laboratory Diagnosis. Dr.T.V.Rao MD
Identification of C.albicans • Mixed culture of C. neoformans and C. albicans on bird seed agar (Guizotia seeds) showing the distinctive brown colonies of C. neoformans, due to the selective absorption of pigment from the media, compared to the white colonies of C. albicans. Dr.T.V.Rao MD
1Microscopic morphology of C. neoformans showing encapsulated budding, yeast cells. No pseudo hyphae are produced.0
C. neoformans on Sabouraud's dextrose agar • C. neoformans on Sabouraud's dextrose agar showing typical dark cream coloured, smooth, moist, shining and mucoid colonies. Dr.T.V.Rao MD
Immune competent - Fuconazole,Itraconazole Immune Deficient – Amphotericin B Flu cytosine AIDS patients are not totally cured , Relapses are frequent with fatal outcome. Rapid resistance with Fluconazole. Avoid contact with Birds Treatment Dr.T.V.Rao MD
Prevention • Fluconazole prophylaxis • Active immunization- cryptococcal GXM-tetanus toxoid conjugate vaccine- in animal models, no human trials • Monoclonal antibodies- would require repeated injections • Avoid high risk environments
HIV Lymphoproliferative disorders Sarcoidosis Corticosteroids Hyper IgM or IgE syndrome Monoclonal antibodies (infliximab) SLE CD4 T-cell lymphoma (idiopathic) Diabetes Organ transplant Peritoneal dialysis Cirrhosis 20% without HIV have no underlying comorbidity Epidemiology
Created by Dr.T.V.Rao MD for Medical and Paramedical students in Developing World • Email • doctortvrao@gmail.com Dr.T.V.Rao MD