Download
1 / 15
150 likes | 268 Views
Care of the Seriously Ill Child in an Adult ICU in an Emergency Situation. APPENDIX 3. Children are Different. ESTIMATING WEIGHT. NORMAL VALUES. Infants are dependent on good diaphragmatic function.

E N D
Care of the Seriously Ill Child in an Adult ICU in an Emergency Situation APPENDIX 3
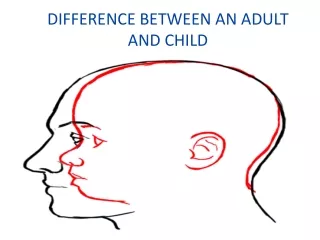
Children are Different ESTIMATING WEIGHT NORMAL VALUES
Infants are dependent on good diaphragmatic function • The infants diaphragm inserts more horizontally in conjunction with their ribs, which causes lower rib retraction especially when supine.
Anatomical factors which impact upon the child’s spontaneous ventilation • The infant’s chest wall is more compliant / less rigid due to cartilaginous sternum and ribs. • The inter-costal muscles do not assist the infant in elevating the rib cage but act a a stabiliser.
Differences in the infants respiratory system compared to an adults Large amounts of lymphoid tissue Larynx higher –risk of aspiration Large Tongue – airway obstruction Diaphragm & intercostal muscles have fewer type 1 muscle fibres - adaptions for sustained activity, hence tire earlier Alveoli still developing in size and numbers (95%) Greater oxygen consumption due to higher BMR Airways shorter & narrower encircled by cricoid cartilage – less support Mucous membranes loosely attached airway oedema greater
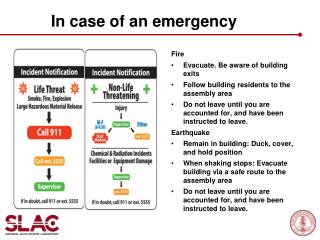
AssessmentAirway • Stridor suggests upper airway obstruction - croup • Grunting is exhalation against a partially closed glottis to increase end expiratory pressure • Opening manoeuvres should be used in a child with a compromised airway – consider use of adjuncts (Guedal, nasopharngeal or intubation) • N.B. A child with a compromised airway may quickly become obstructed if distressed
Bag Valve – Mask Ventilation • If hypoventilating with slow respiratory rate or weak effort support is required via bag-valve mask device • The mask should extend from bridge of nose to cleft of chin, enveloping nose & mouth but avoiding compression of eyes. • Face mask application with one hand as head tilt-chin lift manoeuvre is performed
Airway Adjuncts & Sizing From the incisors to the angle of the mandible Avoid pressure on the soft tissues of the neck which could cause laryngeal/ tracheal compression Measure from the tip of the nose to the tragus of the ear
Endotracheal Tube Sizing Endotracheal tubes diameter size: • <1 year = 3.0, 3.5, 4.0 • >1 year = age / 4+4; i.e. 4 years / 4+4=5.0 plus 4.5 & 5.5 • Oral length = Age / 2 + 12
Ventilation • Respiratory rates – 20-30bpm • Inspiratory time – • Usually starting at 0.7 sec for infants to 1 sec • Inspiration pressure – • Normal healthy lungs = 16-18 cmH20 • Stiff non-compliant lungs = 30-40 cmH20 to generate similar tidal volumes • Start at 20-25 cmH20
Ventilation • Pre-set positive end expiratory pressure (PEEP) = 3-5 cmH20 • Tidal volumes (TV) • 5-7ml/kg neonates • 7-10ml/kg children • Use adult ventilation circuit > 15kg
Assessment Circulation • If signs of shock – fluid bolus 10-20 ml/kg 0.9% saline • Start inotropes 50-60ml/kg administered in conjunction with volume replacement • Warm shock • Start with dopamine • Add adrenaline or noradrenaline • Cold shock • Start with dobutamine • Add adrenaline or noradrenaline Intraosseous placement
Assessment • Disability: Conscious level, behaviour • Normal, lively, irritable, lethargic • AVPU / GCS pupillary signs & posture • A child who only responds to PAIN has GCS of 8 or less and • THE AIRWAY IS AT RISK • Exposure: • Keep normothermic • Rash, fever, consider anaphylaxis
Calculations Fluids / Feeds • Calculations Enteral Feeds: • 3-6 months old 120ml/kg/day • > 6 months old use above IV fluid calculation • Example: 35kg child: • Method 1 = (10 x 100) + (10 x 50) + (15 x 20) = 1800ml/day = 75ml/hr • Method 2 = (10 x 4) + (10 x 2) + (15 x 1) = 75ml/hr • Dextrose 5% 0.45% saline (KCL 10mmol/500ml)
Summary • The most common cause of illness in infancy and childhood is acute disease of the respiratory tract. • The younger the child / infant the more susceptible they are to respiratory difficulties due to anatomical differences • Adopting a systematic approach to the stabilisation of seriously ill children will allow practitioners to approach their care with confidence.