Download
1 / 61
650 likes | 1.37k Views
Robotic Total Mesorectal Excision Oscar I. Moreno Ponte MD. Objectives. 1. Discuss overview of robotic surgery. 2. Describe evolution of robotic surgery 3. Discuss applicability of robotic surgery in colorectal surgery.

E N D
Robotic Total Mesorectal Excision Oscar I. Moreno Ponte MD
Objectives 1. Discuss overview of robotic surgery. 2. Describe evolution of robotic surgery 3. Discuss applicability of robotic surgery in colorectal surgery. 4. Review oncological and clinical outcomes of laparoscopic mesorectal excision. 5. Review oncological and clinical outcomes of robotic mesorectal excision.
Robotic Surgery …”Developed to overcome the limitations of minimally Invasive Surgery and to enhance the capability of open surgery”…
Chronological Events First Remote Cholecystectomy. The Lindbergh Operation Dr. Jacques Marescaux and Dr. Michel Gagner New York, September 2001.
History of Robotic Surgery In 1985, PUMA 560 CT guided brain biopsy A robot with improved absolute positioning accuracy for CT guided stereotactic brain surgery. Kwoh, Y. Et all. Engng, Feb 1988, 35(2), 153–161.
History of Robotic Surgery In 1988, The PROBOT PROBOT-A Computer Integrated Prostatectomy System Mei, Q. Et all. LNCS, 1996, Volume 1131/1996, 581-590
History of Robotic Surgery In 1992, The ROBODOC The ROBODOC Clinical Trial: A Robotic Assistant for Total Hip Arthroplasty. Spencer. E.H. Et all Ort Nur, 1996, VOL 15; NUMBER 1,Pag 9-14
History of Robotic Surgery In 1994, ZEUS Robotic Surgical System Robots Helping Surgeons: The da Vinci and ZEUS System By FDA
History of Robotic Surgery In 2000, The da Vinci Surgical System Robots Helping Surgeons: The da Vinci and ZEUS System By FDA
Chronological Events - 1997, Dr Tommaso Falcone, Cleveland Clinic; Successfully reconnection of fallopian tubes using ZEUS surgical system. - 1998, Dr Friedrich Wilhelm, Leipzig Heart Center; First Robotic Assisted heart bypass using da Vinci surgical System. - 1999, Dr. Randall Wolf and Dr. Robert Michler, The Ohio state university; First Robotic Assisted heart bypass in USA. - 2001, Dr. Jacques Marescaux and Dr. Michel Gagner; first remote cholecystectomy. - 2008, Dr. Mohan S. Gundeti, University of Chicago; First robotic pediatric neurogenic bladder reconstruction. - 2009, Dr. Stuart Geffner, Santa Barbara Medical Center, Ney Jersey; the first all-robotic-assisted Kidney transplant. - 2010, Dr. Borut Gersak, University Medical Centre Ljubljana; first robotic operation at the femoral vasculature
Chronological Events First Fallopian Tube Reconstruction. Successful pregnancy 2 years after reconstruction. Dr Tommaso Falcone; Cleveland Clinic, July 1997.
Chronological Events First Robotic Assisted heart bypass using da Vinci surgical System. Dr Friedrich Wilhelm; Leipzig Heart Center, Germany 1998
Chronological Events First Robotic Assisted heart bypass in USA. Dr. Randall Wolf and Dr. Robert Michler The Ohio State University 1999
Chronological Events 1999….World's first surgical robotics beating heart coronary artery bypass graft (CABG) was performed in Canada by Dr. Douglas Boyd and Dr. Reiza Rayman using the ZEUS surgical robot…. Same year…. the first closed-chest beating heart cardiac hybrid revascularization procedure is performed at the London Health Sciences Centre (London, Ontario)
Chronological Events Robotic assisted Aortobifemoral bypass Dr Willem Wisselink, Vrije Universiteit Medical Center. Amsterdam, The Netherlands 2002
Chronological Events First robotic pediatric neurogenic bladder reconstruction. Dr. Mohan S. Gundeti, University of Chicago 2008
Chronological Events First all-robotic-assisted Kidney transplant. Dr. Stuart Geffner, Santa Barbara Medical Center, New Jersey 2009
Robotic Surgery Application Otolaryngology—Head & Neck Surgery Gastrointestinal Surgery Cardiothoracic Surgery Cardiology and Electrophysiology Urology Gynecology Neurosurgery Orthopedic Pediatric
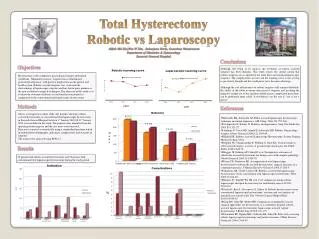
Laparoscopic Surgery Standard of care for most benign and malignant colorectal disease. Less post-operative pain Better Cosmesis Early return of bowel function Shorter hospital stay Without sacrificing oncological clearance.
Laparoscopic Surgery - Shortcomings of laparoscopic surgery Two dimensional view Dexterity of instruments within the abdominal space Fixed instruments tips with 4 degree of freedom Possible misalignment of hands and instruments
Robotic Surgery The da Vinci Surgical system was developed to overcome shortcomings of laparoscopy….. Three dimensional imaging Stable camera and operating platform Articulating instruments with 7 degree of freedom Motion scaling and and tremor free movements Ergonomic Comfort
Open Versus Laparoscopic Colorectal Surgery Cancer Treatment Reviews 2008 Vol 34, 498– 504
Open versus Laparoscopic Colorectal Surgery Twelve trials More than 3346 patients No difference in recurrence rate No difference in Cancer related mortality
Open versus Laparoscopic Colorectal Surgery ….” For any stage, 3 year survival and disease free interval are not worse in patients undergoing laparoscopic versus conventional open resection”……
Laparoscopic Vs Open Surgery for rectal Cancer. COLOR II. A randomized clinical trial comparing laparoscopic and open surgery for rectal cancer. - International Clinical Trial - Primary end point: Loco-regional recurrence rate - Secondary end point: Disease free survival, post operative morbidity, quality of life and health economy analysis. “The results and safety of Laparoscopic Surgery in the treatment of rectal cancer remains unknown”
Laparoscopic Rectal Surgery ….”Technical Complexity and long Learning curve can compromise oncologic Outcomes”…..
Laparoscopic Rectal Surgery …”Ninety operation required to achieve oncological safety”….
Robotic Rectal Surgery …” Stable view and precise movements make the Robot specially appropriate for manipulation of tissue in a closed and fixed space”… …” We believe that robotics could be relevant in the treatment of rectal cancer”….
Robotic Colorectal Surgery Relatively new approach…. SURG ENDOSC 2002 Vol. 16, Number 8, 1187-1191
Robotic Colorectal Surgery Relatively new approach…. DIS COLON RECTUM 2002 Vol. 45, Number 12, 1689-1696
Robotic Colorectal Surgery - Robotic Assisted Technique for the mobilization of the bowel - Three arm da Vinci System - Three-trocar Technique - Division of the Mesentery and Anastomosis performed with standard laparoscopic assisted technique. - Operative time 228-340 (180) - No Complication - Expected postoperative course
Robotic Rectal Surgery Operative Technique Hybrid Technique: Laparoscopic mobilization of the colon and Robotic TME Totally Robotic Anterior Resection A. Pagazzi et all; Surg Endosc 2006 Vol 20, 1521-1525 M. Hellam et all; Ann of Surg Onc 2007 Vol 14, 3168-3173
Robotic Rectal Surgery LAR 80 (55.9%) CA 32 (22.4%) APR 31 (21.7%) Sphincter preservation achieve in 78.3 % Diverting Ileostomy 63% Operative time 297 min EBL 283 ml (0-6000 ml) Conversion to open 4.9% Ann Surg Oncol 2010 Vol 17:1614–1620
Robotic Rectal Surgery Overall anastomotic leak 10.5% - Tumor Location >7 cm from the anal verge 9.3% - Lower tumors 16.4% Overall Pelvic Septic Complications abscess and leakages 16%
Robotic Rectal Surgery Oncologic Outcomes Negative distal and circumferential margins 99.3% Mean number of harvested lymph nodes 14.1 Complete pathologic response 19.3% No Port site recurrence Total Recurrence 13 patients; Distant-only Mets 7.7% Local combined with distal Mets 1.5% No Local-only recurrence Disease free Survival at 3 years 76.6% Three year overall Survival rate 77% Ann Surg Oncol 2010 Vol 17:1614–1620
Robotic Rectal Surgery “All circumferential and Distal resection margins were negative The medial number of harvested lymph nodes was 14.5”
Robotic Vs Laparoscopic TME Ann Surg Oncol 2009 Vol 16:1480–1487
Robotic Vs Laparoscopic TME Ann Surg Oncol 2009 Vol 16:1480–1487
Robotic Vs Laparoscopic TME Ann Surg Oncol 2009 Vol 16:1480–1487
Robotic Vs Laparoscopic TME Ann Surg Oncol 2009 Vol 16:1480–1487