Download
1 / 39
480 likes | 1.32k Views
Hysteroscopic section of T-Y shaped uterus. Op. Dr. Hüsamettin USLU Brüksel Tüp Bebek Merkezi. Case 1 ( Y-shaped uterus). 38 yrs old (2007) 19 yrs of marriage 4 spontaneous abortions (1991, 1994, 1995,1997) 4 IVF trials (2001, 2002, 2005, 2006)

E N D
Hysteroscopic section of T-Y shaped uterus Op. Dr. Hüsamettin USLU Brüksel Tüp Bebek Merkezi
Case 1 ( Y-shaped uterus) • 38 yrs old (2007) • 19 yrs of marriage • 4 spontaneous abortions (1991, 1994, 1995,1997) • 4 IVF trials (2001, 2002, 2005, 2006) • Diagnostic Hysteroscopy – minimally arcuate(2006) • 2007 38 W term delivery after hysteroscopic Y-shape uterus section and ART
Effect of diethylstilbestrol on reproductive function • DES is a synthetic nonsteroidal estrogen used for threatened abortion • Banned in 1971 due to association between vaginal clear cell adenocarcinoma, uterine anomalies and in utero DES exposure • Currently, the youngest women exposed to DES are 37 yrs old • Induces uterine malformations, including hypoplastic cavity, T-shaped uterus, constriction bands, irregular borders
Approximately 70% of women exposed to DES in utero had uterine abnormalities detected on hysterosalpingography. The most common abnormality was hypoplastic T-shaped cavity (31%). Kaufman RH. et al. Am J Obstet Gynecol 1980
Although prescription was prohibited after the publication of papers by Herbst et al (1970, 1974...), an estimated 4 million women had already taken the drug. • The risk does not depend on the total dose absorbed but on how early was exposure to DES.
Higher percentage of premature births, ectopic pregnancies and in utero fetal deaths are reported in the DES group. • Spontaneous miscarriages and late abortions were found to be significantly higher in the DES group. Herbst et al. Am J Obstet Gynecol 1981 Ludmir et al. Am J Obstet Gynecol 1987
50 women with primary infertility and presumed in utero diethylstilbestrol (DES) exposure and in 50 age-matched controls. Uterine deformities and endometriosis were more frequent in the DES-exposed women than the controls. When managed from one to four years, only 4% of DES-exposed women with primary infertility conceived (with no conceptions resulting in a viable fetus) as compared to 44% of controls. Berger MJ, Alper MM J Reprod Med 1986
Endocervical canal width was one third that of unexposed uteri • Myometrial thickening produced indentations into the cavity • Reduction in menstrual blood loss may be attributed to the smaller endometrial cavity area as well as a reduction in the endometrial thickness Kaufman RH et al Am J Obstet Gynecol 1984 Haney AF et al Fertil Steril 1979 Salle B et al Human Reproduction 1996
9x increase in ectopic pregnancy • 2x spontaneous abortion • 2x preterm delivery • 1.5x lower term delivery • 1.3x lower live birth rate
Etiology of implantation failure • Implantation failures considered to be a result of uterine hypoplasia (due to mechanical reasons uterus can not distend enough) • Uterine PI are significantly higher in DES group and blood flow does not increase in the luteal phase (functional reasons) • Or BOTH
Two hypothesis for functional reasons • DES could introduce a histological anomaly in uterine arteries OR uterine arteries may lack sensitivity to estradiol due to a reduction in the number of receptors. Pre-eclampsia was twice in DES group Trophoblastic invasion can not occur PI values increses in the luteal phase Mittendorf and Williams Lancet 1995
Average values of uterine and arcuate artery PI of unexposed uteri tended to decrease significantly in the luteal phase • However, uterine and arcuate artery PI of uteri exposed to DES remained stable throuhout the cycle • Wise to use anticoagulant therapy
It should be noted that classic small T-shaped uterine cavity also has been found in women who were not exposed to DES in utero - congenital mullerian malformation - uterine infection - uterine instrumentation Rennell CL. AJR Am J Roentgenol 1979
Treatment • Hysteroscopic metroplasty ± cerclage IUD + hormonal support + intracavitary balloon • Assisted reproductive techniques these patients have a similar number of oocytes retrieved, fertilized and embryos replaced as patients with tubal factor infertility reduce the number of embryos transferred to avoid the complication multiple pregnancy in the already compromised uterus • Anticoagulant therapy ( low dose aspirin, nadroparine calcium....)
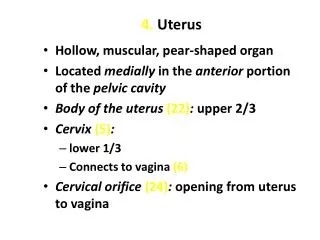
Cylindrical uterine cavity Bulging uterine side walls Triangular, symmetric cavity
Case 2 ( T-shaped uterus) • 28 yrs old • IUI x 3 (1999) • IVF (2000): 20 oocytes, 3 ET, 6 cryo • Thaw ET x 2 • IVF (2002): 10 oocytes, 3 ET, 3 cryo • Thaw ET x 1 • IVF (2003): 10 oocytes, 4 ET, 3 cryo • Thaw ET x 1 • Diagnostic hysteroscopy (2004): narrow cavity, long cervical canal • IVF (2005): 10 oocytes, 4 ET (PGD) • IVF (2006): 13 oocytes, 4 ET IVF x 5 Thaw ET x 4 6 weeks abortion x 2
Hysteroscopic section of T-shaped uterus • 36 yrs of age • Endometrial line: 6.2 mm (follicular phase, day 14) • 2007 hysteroscopic metroplasty + IVF ( 2 blast ET) • 35 W c/s
IUD + hormonal support + intracavitary balloon • Estradiol hemihydrate (8 mg/day) 0 6 weeks of the procedure • Lynestrenol (5 mg/day) 4 6 weeks • IUD ( multiload ) until 4th week • Intracavitary balloon on the 4th week
Intracavitary balloon • Foley catheter ( 12f ) total of 6 cc serum physiologic for 1 minute after extraction of the IUD
Cervical cerclage • DES exposed cervix may be predisposed to incompetency because of an increase in the ratio of smooth muscle to collagen, structural changes in collagen fibrils and decreased elastin content. • Although some uncontrolled studies advocating prophylactic cerclage, most authors consider to limit this procedure to standard clinical indications Michaels et al Obstet Gynecol 1989 Levine et al Am J Obstet Gynecol 1993
Hysteroscopic metroplasty in DES exposed uterus and subsequent reproductive performance • 8 patients • Prior to metroplasty - recurrent pregnancy loss (6 patients) - primary infertility (2 patients) • After metroplasty - 3 term deliveries in 3 women Nagel TC, Malo JW Fertil Steril 1993
Eight women (aged 27-43) with reproductive dysfunction who were diagnosed by hysterosalpingogram and hysteroscopy as having a 'T-shaped' uterus were operated by hysteroscopy.
Hysteroscopic metroplasty in DES-exposed and hypoplastic uterus: a report on 24 cases • It is an effective procedure in the case of recurrent abortion(88%12.5%) • It improves the rate of term delivery (3%87.5%) Garbin et al. Human Reproduction 1998
Effect of hysteroscopic metroplasty for T-Y shaped uterus on pregnancy outcome(Brüksel Tüp Bebek) • 2004 - 2008 • Total of 41 (14 primary infertility, 27 recurrent pregnancy failure) subjects underwent hysteroscopic section of T-Y shaped uterus
Outcome prior to hysteroscopic metroplasty(Brüksel Tüp Bebek) 2 abortions + 30W live delivery 1 ectopic + 29W live delivery 5 abortions + 32W live delivery 3 abortions + 32W live delivery
after hysteroscopic metroplasty Live birth 24,4%
Conclusion • Hysteroscopic metroplasty for T-Y shaped uterus seems to be an operation that improves the rate of live birth rate with a history of - primary infertility - recurrent abortion - preterm delivery • in order to evaluate the efficiency of this technique, randomised trials should be undertaken with larger series
Case 3: Hysteroscopic enlargement of unicornuate uterus 38 years old (2009) 5x IVF 2x SA Endometrial lining: 6.1 mm Hysteroscopic metroplasty IVF (2 blast ET) 29 weeks of singleton gestation (ongoing)