Download
1 / 20
210 likes | 222 Views
NEUROPSYCHOLOGY 3. The Neurobiology of Emotional Behaviours and Stress. Dr. Malcolm Hughes. Of all the terms that psychologists commonly use, ‘ emotion’ may be the most difficult to define.

E N D
NEUROPSYCHOLOGY 3.The Neurobiology of Emotional Behaviours and Stress Dr. Malcolm Hughes
Of all the terms that psychologists commonly use, ‘emotion’ may be the most difficult to define. Even though the term ‘emotion’ is poorly defined, the behaviours generally associated with it e.g. escape and attack, are too important to ignore. When we observe people who have become “emotional” their behaviour is undeniably different from usual – often, such behaviours are vigorous and persistent (Thompson, 1980). Role of the Autonomic Nervous System (A.N.S.) in Emotional Behaviours Two parts of the A.N.S. govern behaviour: a) the sympathetic nervous system (S.N.S.) – prepares the body for intense, vigorous activity. b) the parasympathetic nervous system (P.N.S.) – increases digestion and other processes associated with relaxation. These systems are active at all times, although at times, one may be more active than the other.
Arousal of the S.N.S. and P.N.S. The S.N.S. is activated, not by stimuli themselves but rather by the way an individual interprets those stimuli. e.g. One group of boys given a task and told it was a test – responded with increased heart rates; Second group given the same task but told it was a game – reacted with decreased heart rates (Darley & Katz, 1973). In a study by Malcuit (1973), people who received inescapable shocks and knew the shocks were inescapable had decreased heart rates – a typical parasympathetic response to uncontrolled distress. Those who were misled into thinking they could escape the shocks had increased heart rates.
Emotions, Autonomic Responses and Health Today there is little doubt that stressful experiences and thoughts of despair can increase the risk of many kinds of illness and disease. Conversely, social support, sense of humour and other positive emotions can prolong survival or improve the quality of like for those with serious illnesses. Appreciating the psychological factors in health is relatively new in Western medicine – trend more towards behavioural medicine or medical psychology: - such areas focus on diet, drinking and smoking habits, exercise and other behaviours on people’s health, including variations in emotional states. The A.N.S. and Psychosomatic Illness Individual’s A.N.S. responsiveness is highly consistent over time but will vary from one person to another. Some show stronger and quicker sympathetic responses – such individuals also tend to: show more emotional expression are generally more gregarious, more impulsive and less patient.
Those with a highly responsive S.M.S. also tend to be vulnerable to heart disease and other medical disorders. In such psychosomatic illnesses the probability of getting the disease or recovering from it depends largely on the psychological make-up of the individual e.g. personality and/or experiences. The role of the A.N.S. in Ulcer formation Ulcers can form in various ways, but those who experience work-related stress are believed to be particularly vulnerable. Proved in animal studies during the 1950’s and 1960’s – the “executive” and “passive” monkey experiments (Brady et al, 1958; Foltz & Millett, 1964). Evidence indicates that ulcers do not form during stress periods, but usually during periods following stress (Desiderato, et al, 1974). The period of stress greatly activates the S.N.S. During the less stressful periods, the P.N.S. rebounds, releasing an excess of digestive juices that damage the lining of the stomach and intestines.
Digestive secretions are not the full explanation – during periods of stress and the period immediately following, the stomach makes intense contractions; - Has the effect of breaking up the mucus lining of the stomach, thereby exposing more of the stomach wall to the digestive secretions (Garrick, 1990). The Impact of Chronic Stress on the Immune System The body’s response to chronic stress differs from its response to transient episodes of stress; there is a different set of responses to more severe and prolonged periods of stress. Stressors excite both the S.N.S. and an axis comprising the hypothalamus,pituitary gland and adrenal cortex. The hypothalamus induces the anterior pituitary gland to secrete adrenocortico-tropic hormone (A.C.T.H.). This in turn stimulates the secretion of cortisoland other steroid hormones. Cortisol has the effect of elevating blood sugar and enhancing metabolism; in the medium to long-term, this causes a shift away from the synthesis of proteins, including those proteins necessary for the immune system. Thus, in the long term, this causes a weakening of the immune system making the individual vulnerable to a variety of illness conditions.
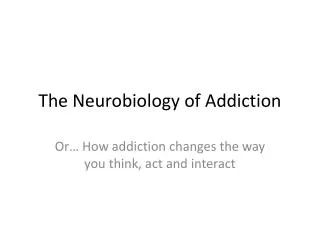
Pathways for the effect of emotional stress through the anterior and posterior hypothalamus (Stoll, 1983).
Now recognised that the nervous system has considerable control over the immune system – psychoneuroimmunology(O’Leary, 1990, Kiecolt-Glaser, 1993, 1998). Certain prolonged stressful events can release endorphins - decrease pain but suppress blood levels of natural killer (N.K.) cells (which naturally attach to tumour cells and cells infected with viruses). If N.K.cell levels decrease, the individual is more vulnerable to infection; if they develop a tumour, the tumour grows more rapidly. The relationship between stress, the immune system and health change in humans remains partly unclear e.g. most rat tumours are caused by viruses, while the vast majority of human ones are not. Also, depression often correlates with impaired responses to the immune system (Weisse, 1992), yet chronically depressed individuals have virtually normal life expectancies (Stein et al, 1991). Still unclear as to whether particular types of stress or stressful life episodes have a more adverse effect than others.
The Limbic System and Emotional States Emotional behaviour dependant upon structures within the limbic system – include the: - hypothalamus, hippocampus, amygdala, olfactory bulb, septum + parts of the thalamus and cerebral cortex. Therefore, subcortical areas appear to generate emotional behaviours – the cerebral cortex directs those behaviours towards appropriate targets as well as trying to suppress them. MacLean (1970) – evidence that the limbic system is important for emotion based on observations of individuals suffering from temporal lobe epilepsy - most with T.L.E. have no particular emotional experiences with their episodic seizures. However, a substantial majority experience the following: • Aggressive impulses • Dissociation of experience similar to multiple personality (Schenk, 1981) • Uncontrollable laughter (Swash, 1972) • Sexual arousal (Rémillard et al, 1983) • Feeling of extreme bliss (sense of oneness with the universe)
Within the limbic system, MacLean distinguished three circuits: a) amygdala & hippocampus – involved with self-preservation b) cingulate gyrus (cerebral cortex) & septum – associated to sexual enjoyment. c) hypothalamus and ant. thalamus – believed to be important for co-operative social behaviour (larger in primates than in other animals). Fear and Anxiety With few exceptions, fear is either learned or modified by experience – people with post-traumatic stress disorder (P.T.S.D.) show an enhanced startle response compared to others (Shalev et al, 1992). The startle response can be used to gauge levels of fear or anxiety – studies indicate that if an animal (incl. humans) have learned an association between some stimulus and shock, that stimulus becomes a “fear signal”. e.g. presenting that stimulus just before a loud noise enhances the animal’s response to the noise – links to phobias.
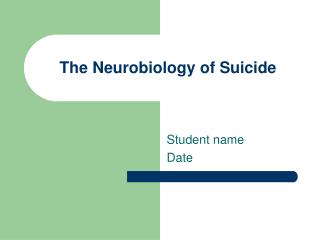
The Amygdala and its connections relevant to the leaning of fears and anxieties
Key area associated with fear is the Amygdala. – a rat with damage to the amygdala shows a normal startle response after a loud noise, but no enhanced startle response to the combination of the “fear signal” plus loud noise (Phillips & LeDoux, 1992). In general, such animals neither learn new fears nor retain learned fears acquired before brain damage (Kim & Davies, 1993). The amygdala sends its output to various parts of the brain: Its connections to:- Hypothalamus – controls autonomic fear response e.g. increased blood pressure. Hindbrain – controls flinching, freezing and similar skeletal responses. Suggestion that there might also be links to the Pons and the Medulla. Most incoming information to the amygdala comes directly from the thalamus, not as suspected the cerebral cortex – i.e. amygdala does not rely on highly detailed information, but gets the information very rapidly. Likely that this might link some fears with pain – fear conditioning.
Anxiety-Reducing Drugs Anti-anxiety drugs – barbiturates (habit forming) or, more recently, the benzodiazepines (Valium, Librium, Xanax)– Have the effect of relaxing muscles, induce sleep and decrease liklihood of convulsions (anti-epileptic effect). During 1980’s, benzodiazepine receptors discovered (GABA receptors). The brain possess at least two major categories of such receptors: GABAA - (tend to decrease anxiety) andGABAB receptors. GABA receptor has a chloride channel – when open chloride ions cross the membrane into the neurone – inhibits the synapse. Surrounding the chloride channel are four units, three of which (α) also contain the benzodiazepine receptor. When attached, benzodiazepine molecule alters the shape of the receptor so that GABA attaches more readily: - results in greater flow of chloride ions across the membrane, ultimately adjusting the anxiety levels of the person.
Synthesis of Serotonin Tryptophane 5-hydroxytryptophan Serotonin (from diet) (5-hydroxytryptamine) Serotonin Synapses and Aggressive Behaviour In terms of emotional behaviour, aggression is recognised as a characteristic found in all species Although it is unlikely that a single neurotransmitter system controls aggression, evidence indicates that serotoninis implicated: i.e. a low serotonin release = with rise in aggression Research evidence – people with history of violent behaviour (incl. violence towards self) have lower-than-average serotonin turnover. Those who have attempted or succeeded in committing suicide are found to have low levels of 5-HIAA (5-hydroxy indole acetic acid, a serotonin metabolite) in the blood, C.S.F. and urine – suggests lower than normal release of serotonin.
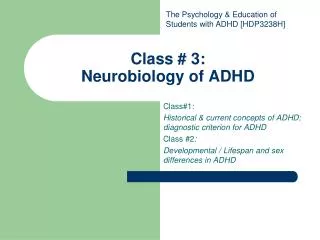
Levels of 5-HIAA in the CSF of depressed people according to suicide attempts (Roy, DeLong & Linnoila, 1989).
Such individuals also have more %-HT2 (serotonin2) receptors than usual in the cerebral cortex – possibly brains means of compensating for decreased serotonin release. Serotonin turnover also depressed in those convicted of arson and violent crimes. Hypothesis suggests that serotonin synapses INHIBIT behavioural impulses that might lead to punishment or other unfavourable outcomes. i.e. when serotonin turnover is HIGH, have restrained behaviour; when serotonin turnover is LOW, have impulsive behaviour, incl. violent outbursts. Now recognised that the measurement of serotonin turnover could be used to predict the probability of a person with low serotonin levels repeating specific actions – 84% probability. e.g. person attempting suicide likely to repeat the act, possibly with fatal consequences within 5 years (Roy, DeLong & Linnoila, 1989). Also, person convicted of manslaughter or arson, more likely to repeat crime after release from prison (Virkunnen et al, 1989).
Serotonin is particular neurotransmitter whose fluctuating presence in the brain goes beyond the conditions considered so far. As already demonstrated, it is linked to depressive episodes, when serotonin levels decrease as well as aggressive or violent behaviours Evidence also points to the involvement of the chemical in obsessive – compulsive disorders. Among such sufferers, many respond well to the drugs clomipramineand fluvoxamine – both inhibit the reuptake of serotonin by the pre-synaptic neurone i.e. the drugs prolong the effects of serotonin at the synapse. Conversely, drugs that inhibit serotonin synthesis tend to aggravate the symptoms of obsessive-compulsive disorder. In view of these findings, there exists a strong case for suggesting that measurement of serotonin levels could be used as a predictor of some forms of human behaviour or mental disorder. Whether or not anyone should use serotonin measures in such a way raises ethical and legal issues – after all, predictions based on serotonin turnover remain far from perfect.