Download
1 / 47
470 likes | 474 Views
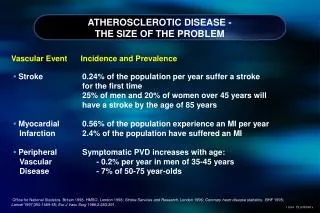
Explore the latest approaches to modify lipids and lipoproteins for the prevention of atherosclerotic vascular disease. Learn about new developments in LDL reduction, inflammation reduction, and raising HDL levels.

E N D
Novel therapies for the prevention of atherosclerotic vascular disease Slidesprepared and presentedby John Kastelein, MD Academic Medical Centre Amsterdam, The Netherlands At CV Risk master classes 2013
Novel Approaches to Modify Lipids and Lipoproteins • Low DensityLipoprotein • High DensityLipoprotein • TriglycerideRichLipoproteins • Inflammation • Lipoprotein a
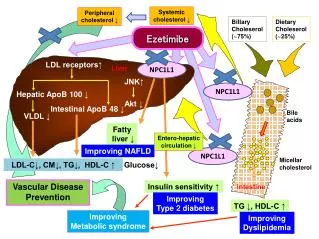
New Approaches to LDL Reduction What is in development? • Cholesterol Absorption Inhibitors • SqualeneSynthase (SSI) inhibitors • Apo B mRNA antisense drugs • Microsomal Triglyceride Transfer Protein (MTP) inhibitors • Thyroxin Receptor Agonists • PCSK9 Inhibitors
PCSK9 LOF Mutations No Nonsense Mutation (N=3278) 30 20 10 0 50th Percentile 88 percent reduction in the risk of CHD 12 8 4 0 Frequency (%) 0 50 100 150 200 250 300 Coronary Heart Disease (%) PCSK9142x or PCSK9679X (N=85) 30 20 10 0 28 percent reduction in frequency No Yes 0 50 100 150 200 250 300 PCSK9142x or PCSK9679X Plasma LDL Cholesterol in Black Subjects (mg/dL) Adapted from Cohen JC. N Engl J Med 2006;354:1264-72; ARIC=Atherosclerosis Risk in the Community
Loss of Function PCSK9 Mutations • Only a small number of patients who are homozygous (or compound heterozygotes) for PCSK9 have been discovered and studied. • These patients appear to have: • Very low LDL-C levels (~10-20 mg/dL) • Relatively low TG levels • Normal HDL-C levels • These patients have no other health problems
FamilialHypercholesterolemia Mabuchi H et al. Circulation 1989;79:225–232.
FH in the Netherlands: ScreeningbetweenJanuary 1994 and December 2010
FH in the Netherlands: ScreeningbetweenJanuary 1994 and December 2010
The Use of a PCSK9 Monoclonal AB in heFHPatients A Randomized, Double-Blind, Placebo-Controlled Trial of the Safety and Efficacy of a Monoclonal Antibody to PCSK9, REGN727/SAR236553, in Patients with Heterozygous Familial Hypercholesterolemia on Stable Statin Dose With or Without Ezetimibe Therapy Evan A. Stein, Dan Gipe, Jean Bergeron, Daniel Gaudet, Robert Weiss, Robert Dufour, Richard Wu, Robert Pordy. Lancet, May 2012
The Use of a PCSK9 Monoclonal AB in heFHPatients: Goal Attainment
The Use of a PCSK9 Monoclonal AB in heFHPatients: SecondaryResults
FromStableCoronaryDisease To Acute CoronarySyndromes
NovelStrategiesfor the Management of Acute CoronarySyndromes
The Unmet Need: highest risk early after ACS: Inflammation drives recurrent plaque rupture Cumulative rate MACE (%) Stone NEJM 2011 Rogers JIMG 2010 Fused FDG-PET/CT Image • High residual risk despite statins, PCI • Many events are due to rupture of inflamed, vulnerable plaque • ACS is an inflammatory syndrome • Systemic Inflammation • Multifocal vascular inflammation
Novel Approaches to Modify Lipids and Lipoproteins • Low DensityLipoprotein • High DensityLipoprotein • TriglycerideRichLipoproteins • Inflammation • Lipoprotein a
New Approaches for Reduction of Inflammation What is in development? • Interleukin 1-beta antagonists • Interleukin 12-antagonists • Phosphodiesterase E4 inhibition • Lipoprotein Associated Phospholipase A2 inhibition • CRP mRNA antisense drugs • Anti-ox-LDL antibodies and vaccinations • P38 MAPK inhibitors (Losmapimod) • JAK 1-3 inhibitors • Anti-ox40 and CTLA4 monoclonal antibodies • Oxidized phospholipids (VBL)
The Balance of IL-1 and IL-1Ra :Contribution to Human Disease Pro-Inflammatory Anti-Inflammatory IL-1b IL-1Ra NLRP3 cryopyrin Inflammasome IL-1R Severe Imbalance (Inflammasome mutations) CAPS, MWS, NOMID Moderate Imbalance Psoriasis, contact hypersensitivity syndromes Gout, inflammatory arthritis, Crohn’s, Ulcerative colitis Autoimmune Disorders, thyroiditis Mild Imbalance Atherosclerosis, Diabetes
Novel Approaches to Modify Lipids and Lipoproteins • Low Density Lipoprotein • High Density Lipoprotein • Triglyceride Rich Lipoproteins • Inflammation • Lipoprotein a
New Approaches for Raising HDL What is in development? • Cholesterol Ester Transfer Protein (CETP) inhibitors • ER-Niacin / Laropiprant combination • ApoA1 based strategies • LCAT replacement strategies • ABCA1 agonists / miR-33 inhibition • LCAT agonists • Bile-acid based strategies
Where to Intervene inHDL-C Metabolism? Hovingh et al. Current Opinion in Lipidology 2005
New Approaches for Raising HDL What is in development? • Cholesterol Ester Transfer Protein (CETP) inhibitors • ER-Niacin / Laropiprant combination • ApoA1 based strategies • LCAT replacement strategies • ABCA1 agonists / miR-33 inhibition • LCAT agonists • Bile-acid based strategies
ApoA1 Based Therapies • ApoA1 Mimetics, such as APL-180 Novartis • Full-length ApoA1, such as ApoA1 Cerenis Therapeutics • Pre-Beta HDL, as generated by delipidation, HDL Therapeutics Inc. • Reconstituted HDL, CSL Ltd. • ApoA1 Milano MDCO216, The Medicines Company • Trimeric ApoA1, Borean Pharma and now Roche • RVX-208, as developed by Resverlogix • Fx-5A, as developed by Kinemed Inc.
HDL Phospholipids RVX-208 ABC-A1 Cholesterol ApoA-I Protein ApoA-I mRNA Target Cytoplasm ApoA-I Gene Nucleus Hepatocyte RVX-208 Regulates Transcription of ApoA-I mRNA 30
RVX-208 Molecular Target is the BET Protein 801 1 345-457 632-710 74-185 BRD2 BD1 BD2 ET 1 307-419 562-640 34-145 726 BRD3 ET BD2 BD1 1362 600-678 1 349-461 58-159 BRD4 ET BD2 BD1 27-138 500-578 268-380 1 947 BRDT* ET BD1 BD2 • BET proteins contain two bromodomains (BD) • Bromodomains found in many proteins
Crystal Structure of RVX-208 bound to its Target 1.08Å resolution Binding mode reflects existing SAR Multiple high resolution structures Using structural information to identify new chemical scaffolds and optimize leads
CHI-SQUARE Study Design 50 Sites Canada, US, France, Netherlands Core IVUS Lab Montreal Heart Up to 1000 Subjects Screened w/ Baseline IVUS following Acute ACS Event 504 Subjects Randomized N = 126 Placebo N = 126 Low dose N = 126 Mid dose N = 126 High dose Screen Period 2 weeks Therapy Period 5 weeks Observation Period 2 to 5 weeks Long Term Follow-up 6 months IVUS Visit Screening Infusion Visits Interim Visit Follow-Up IVUS Visit Follow-Up Visit
Percent Change in Atheroma Volume with IVUS LDL-C Reduction vs. HDL-C Increasing Therapy P=0.02 REVERSAL ASTEROID APOA-1 Milano 4 4 2.7* 2 Median change in TAV (%) -0.3† -0.8 -4.2 0 Prava 40 mg 18 months Atorva 80 mg 18 months -2 Rosuva 40 mg 24 months -4 ApoA-1 Milano 5 weeks From no change to regression Progression Nissen SE et al. JAMA. 2003 and 2004
ApoA1 Milano • Manufacturing changes require a full re-start of the development of MDCO-216 (= ApoA1 Milano) • Toxicology programme has been completed • Discussion with regulatory agencies on the clinical development are ongoing • Clinical development of MDCO-216 is expected to be initiated in the second half of 2012.
IVUS clinical trial using selective delipidated HDL Step 1 Collected~1 litreof plasma Step 2 Plasma enrichedthrough process Step 3 Re-infused preβenriched plasma • Used patients own HDL • Cholesterol removed fromαHDL to yield preβ-HDL • Preβ enriched plasma isre-infused into patient Walksman R, et al. J Am CollCardiol 2010; 55 : 2727-35.
IVUS Clinical Trial Using Selective Delipidated HDL Treatment arm (N=14) 1:1 randomization (N=28) Control arm (N=14) Day 0 1 2 3 4 5 6 7 8 Week IVUS IVUS Treatment or control plasma infusion Walksman R, et al. J Am CollCardiol 2010; 55 : 2727-35.
Results of the IVUS Clinical Trial Using Selective Delipidated HDL 4 2.8 2 0 -2 -1.73 -4 Change in atheroma volume (mm3) -6 -6.24 -8 Preβ-HDL infusion -10 Control infusion -12 -12.18 -14 Change in totalatheroma volume Change in 10mm most diseased segment Waksman R, et al. J Am CollCardiol 2010; 55 : 2727-35.
New Approaches for Raising HDL What is in development? • Cholesterol Ester Transfer Protein (CETP) inhibitors • ER-Niacin / Laropiprant combination • ApoA1 based strategies • LCAT replacement strategies • ABCA1 agonists / miR-33 inhibition • LCAT agonists • Bile-acid based strategies
LCAT Product Gradient Drives Reverse Cholesterol Transport LDL Small HDL Clearance CETP Kidney LDL-R LCAT SR-BI nascent HDL (small, preβ-HDL) Peripheral tissues mature HDL (large, α-HDL) Liver
New Approaches for Raising HDL What is in development? • Cholesterol Ester Transfer Protein (CETP) inhibitors • ER-Niacin / Laropiprant combination • ApoA1 based strategies • LCAT replacement strategies • ABCA1 agonists / miR-33 inhibition • LCAT agonists • Bile-acid based strategies
De-Repression of ABCA1 by anti-miR-33 as a MechanismforTargetingAtherosclerosis 45
New Approaches for Raising HDL What is in development? • Cholesterol Ester Transfer Protein (CETP) inhibitors • ER-Niacin / Laropiprant combination • ApoA1 based strategies • LCAT replacement strategies • ABCA1 agonists / miR-33 inhibition • LCAT agonists (Daiichi Sankyo) • Bile-acid based strategies (Atheronova) • CAT-2003, the niacin – EPA conjugate (Catabasis)
Conclusion In the next five years, we will prove or disprove that additional LDL lowering with other agents than statins is effective and we will show or not show that the HDL hypothesis is true.