Download
1 / 19
200 likes | 463 Views
14h00 Douleur. Modérateur : S. Hajji-Zarrouk (TN) Prise en charge de la douleur chronique par le MG M. Abdelmoula (TN) Douleurs neuropathiques, nouvelle approche A. Serrie (FR) Thérapie conservatrice du cartilage articulaire A. Laatar (TN)

E N D
14h00 Douleur • Modérateur : S. Hajji-Zarrouk (TN) • Prise en charge de la douleur chronique par le MG • M. Abdelmoula (TN) • Douleurs neuropathiques, nouvelle approche • A. Serrie (FR) • Thérapie conservatrice du cartilage articulaire • A. Laatar (TN) • Comment prendre en charge une fibromyalgie en 2010 ? • A. Laatar (TN)
PRISE EN CHARGE DE LA DOULEUR CHRONIQUE PAR LE MEDECIN GENERALISTE MORCHED ABDELMOULA MLP-ALGOLOGUE ENNASR MEDICAL TUNIS
INTRODUCTION Algos: douleur quelque soit sa cause, son siège et ses caractères. Priorité de l’OMS. La douleur chronique est une entité à part entière. Mieux la comprendre pour mieux la Traiter.
DEFINITION La douleur est une expérience sensorielle et émotionnelle désagréable associée à un dommage tissulaire présent ou potentiel, ou décrite en terme d’un tel dommage. IASP
Quatre composantes: 1- Sensori-discriminative: brulure, décharge électrique…, brève, continue…, intensité, localisation… 2- Affectivo-émotionnelle: désagréable, pénible…, anxiété, dépression. 3- Cognitive: Processus mentaux susceptible d’influencer une perception (la douleur) 4- Comportementale: Manifestations verbales et non verbales (plaintes, mimiques, position antalgique…)
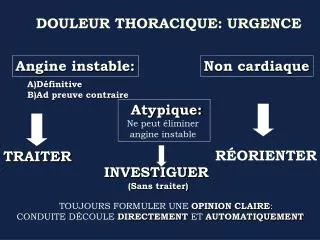
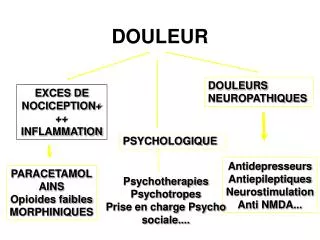
LES TYPES DE DOULEURS 1/ MECANISME PHYSIOPATHOLOGIQUE: • DOULEUR NOCICEPTIVE: traumatisme, brulure, pathologie rhumatismale, cancer • DOULEUR NEUROPATHIQUE : Tumeur de l’apex du poumon, hernie discale, algies post zosteriennes, neuropathies diabétiques… • ORIGINE SINE MATERIA ET PSYCHOGENE : -éliminer une origine organique -stéréotypée (céphalée de tension, fibromyalgie), atypique (description luxuriante, imprécise, variable)
2- DUREE D’EVOLUTION • Aigue: -récente, signal d’alarme, anxiété. -traumatisme, brulure • Chronique: -évolution 3 à 6 mois -destructrice, dépression -douleur maladie -cancer, avulsion plexique, algohallucinose, APZ…
EVALUATION DE L’INTENSITE DE LA DOULEUR Phénomène subjectif et multifactoriel Mesure difficile • Echelles unidimensionnelles: • Echelle numérique • Echelle visuelle analogique (EVA) • Echelle verbale simple • Echelle des visages • Echelles pluridimensionnelle: • Questionnaire douleur de Saint-Antoine (QDSA) • Questionnaire DN4 (douleur neuropathique)
TRAITEMENT PHARMACOLOGIQUE • DOULEUR NOCICEPTIVE Echelle des trois paliers de l’OMS: • PALIER I: EVA 3 ASPIRINE, PARACETAMOL, AINS • PALIER II: 3 EVA 6 ASSOCIATION: CODEINE, DEXTROPROPOXYPHENE, TRAMADOL, AU PARACETAMOL NEFOPAM (ACUPAN*) ADJUVANTS: CORTICOIDES • PALIER III: EVA 6 MORPHINE
DOULEUR NOCICEPTIVE MORPHINE INJECTABLE: CHLORHYDRATE DE MORPHINE MORPHINEVO: SULPHATE DE MORPHINE:skenan*,moscontin* BUPRENORPHINE: temgesic* HYDROMORPHONE: sophydone* PCA: POMPE A MORPHINE: antalgie contrôlée par le patient MORPHINE TRANSDERMIQUE: FENTANYL: durogesic* patch CO-ANALGESIQUES: AINS, CORTICOIDES, NEFOPAM
EFFETS SECONDAIRES DE LA MORPHINE • ASTHENIE, SEDATION: titration • VOMISSEMENT : début du ttt, des doses • DYSPNEE • DEPENDANCE • HALLUCINATION, CONFUSION MENTALE • PRURIT • CONSTIPATION: prévention+++ par laxatifs, bromure de méthylnaltrexone (Relistor*) ANTIDOTE=NARCAN
DOULEUR NEUROPATHIQUE RESISTE AUX ANTALGIQUES USUELS ANTIEPILEPTIQUES: • Carbamazepine: TEGRETOL* • Gabapentine: NEURONTIN*, GABENTIN*, GABA* • Pregabaline: LYRICA* ANTIDEPRESSEURS: • Tricycliques • IRS TOPIQUES LOCAUX: -Capsaicine* PATCH DE LIDOCAINE: -Versatis*
DOULEUR PSYCHOGENE • ANTIDEPRESSEURS: TRICYCLIQUES • RELAXATION • PSYCHOTHERAPIE • ECOUTE++
LES DOULEURS NOCICEPTIVES, NEUROPATHIQUES ET PSYCHOGENES PEUVENT SURVENIR SEULES OU ASSOCIEES CANCER DE LA VESSIE CANCER DE L’APEX DU POUMON ZONA / APZ
LES AUTRES MOYENS THERAPEUTIQUES 1-Stimulations thermiques: • CHAUD: lampes chauffantes (IR), ultrasons… Ex: gonarthrose • FROID: vessie de glace, sprays réfrigérants… Ex: douleurs musculaires 2-Kinésithérapie: 3-Psychothérapie 4-Relaxation 5-Sophrologie
6-Acupuncture 7-Mésothérapie 8-Neurostimulation transcutanée 9-Radiothérapie antalgique 10-Chirurgie
CONCLUSION • Douleur chronique Douleur maladie. • PEC pluridisciplinaire. • Combinaison de plusieurs moyens thérapeutiques (arsenal). • Développement des centres et des consultations de la douleur.