Download
1 / 35
370 likes | 587 Views
High Fidelity Wraparound Process Implications for Schools and Behavioral Health Clinicians. John VanDenBerg, Ph.D. Wraparound or Warparound?. What has been called wraparound has varied widely across the US and Canada.

E N D
High Fidelity Wraparound Process Implications for Schools and Behavioral Health Clinicians John VanDenBerg, Ph.D.
Wraparound or Warparound? • What has been called wraparound has varied widely across the US and Canada. • Key early evaluations of system of care and wraparound showed inconsistent outcomes • The National Wraparound Initiative was formed and successfully brought standards to the field, which has led to a series of scientific studies with consistently positive outcomes
High Fidelity Wraparound Process A Process for Supporting Youth and Families that: • Is defined by ten principles of how the process is implemented; • Is done in four phases and related activities that describe what is to be done; and • Fits the four components of the VVDB theory of change that explains why it works.
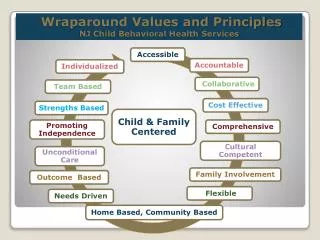
Family Voice and Choice Team Based Natural Supports Collaboration (and Integration) Community Based Culturally Competent Individualized Strengths Based Persistence Outcome Based and Cost Responsible Principles for Wraparound
Engagement & Team Prep Orient family to Wrap Stabilize crises Develop strengths, needs, and culture discovery Engage team members Make meeting arrangements Initial Plan Development Develop a plan of care Develop a detailed crisis and safety plan Implementation Implement the plan Revisit update plan Team cohesiveness - trust Complete documentation and handle logistics Transition Plan for cessation of wrap Conduct commencement ceremonies Follow-up with the family after graduation Phases and Activities of Wraparound
The VVDB Theory of Change • Defines the primary reasons why wraparound can be an effective process • Defines expectations for what we hope to accomplish through wraparound • Many clinicians do their clinical work based on a similar theory of change. However, if their clinical work varies greatly from this theory of change, outcomes may be less than desired
Four Primary Reasons Wraparound Can Be Effective • Families/Youth Identify and Prioritize Their own needs • Self-Efficacy is reinforced at every opportunity • Natural Supports are included in support, planning, and implementation • All systems working with an individual family/youth use a common process and have an integrated plan
The Problem of Engagement in Behavioral Health Services National Health Survey (2008) finds that over 70% of families with a child with SED do not seek, start or complete behavioral health services for their children The primary determinant of success of these services is parental engagement and buy-in Families who need wraparound are often difficult to engage due to their journey through systems -it takes patience and skills to be successful
Research on Engagement Families tell us that there are a number of factors that reduce engagement in the process including Not feeling listened to Past bad experiences with professional staff and experiences reported by other families Treatment goals and plans that do not address the things that are most important to the family and thus feel irrelevant Treatment approaches that do not match the family’s culture In addition, when treatment is provided without full parental engagement, many of youth who do show progress and complete a service component do not have lasting progress
Families raising youth with mental health issues often feel… Embarrassed Fearful Blamed Angry Not Listened To Not Taken Seriously Ashamed Hopeless Misunderstood Ignored Dependent Out of Control J Anthony Irsfeld
Expert vs. Integrated Approaches • The Expert Approach: the responsibility for analyzing the problem, figuring out the causes, and coming up with solutions all rests with the Expert. Tends to rely exclusively on professional knowledge and professional decision making. • The Integrated Approach: Responsibility is shared between the family and the professional(s), with the family identifying and prioritizing needs. Both bring complementary knowledge and strive to combine them to generate positive change, with the family in a final decision making role. J Anthony Irsfeld (adapted by VVDB with permission)
Collaboration and Integration Collaboration: Agencies are familiar with each other’s missions and roles, key staff work with each other at the child/family level, but often retain single system decision making power and planning. Integration: Agencies are familiar with each other’s missions and roles, key staff work with each other at the child/family level, sharing decision making in a team format that includes the family in a lead role, producing a single plan that meets all system mandates and that is owned by the entire team.
Common Assessment Common Registration/Intake INTEGRATED APPROACH INTO WRAPAROUND Single Point of Accountability (Facilitator) Natural Support (Pastor, coach, neighbors) School Child Welfare Common Integrated Plan Peer to Peer Support Juv. Justice Housing Not for Profit Service Agencies Physical Health Mental Health MR/DD
Drift – The Enemy of good wraparound • Wraparound may start with strong demonstration of the Principles and the Phases and Activities, with strong the Action Steps and Core Skills. • Without coaching, certification and monitoring, drift occurs back to old practices. • The VVDB overall materials were a key part of the actual submission to the National Registry of Evidence-Based Practices at a federal level,
Engagement & Team Prep Orient family to Wrap Stabilize crises Develop strengths, needs, and culture discovery Engage team members Make meeting arrangements Initial Plan Development Develop a plan of care Develop a detailed crisis and safety plan Implementation Implement the plan Revisit update plan Team cohesiveness - trust Complete documentation and handle logistics Transition Plan for cessation of wrap Conduct commencement ceremonies Follow-up with the family after graduation Phases and Activities of Wraparound
VVDB defined Action Steps/Skills for the Major Jobs of Wraparound Wraparound Facilitator Peer to Peer Support (Family Support Partner) Supervisor/Coach Action Steps/Skills, once defined, can be coached and learned. VVDB Certification is proving that each staff knows the core Action Steps/Skills and can move onto the “Art” of wraparound.
Many Children and Families in Wraparound have Behavioral Health Needs • Teams consist of the people who can help the family address their needs • Many youth and families in wraparound have BH needs which call for a clinician’s involvement • Often referrals for wraparound come from clinicians • Clinicians in sites that have been doing wraparound report a significant shift in their practice over time and better outcomes for youth and families
Work force implications for Clinicians • Many communities experience a shortage of child-trained clinicians • Wraparound can provide additional information, support, and resources for clinicians to extend their reach with a family/youth and maximize the use of their time, as well as increase effectiveness
Challenges for Clinicians • Not being the “Team Leader” • What to do when the family/youth disagree with professional recommendations • Family cultural practices which may exclude traditional clinical interventions • Lack of system integration and presence of multiple (sometimes competing) planning processes can lead to family/youth alienation with all helping professionals – and at times, blaming of families.
Roles for Clinicians in Wraparound Initially, some clinicians are “less than thrilled” about wraparound, and backlash can occur if wraparound is not understood. However, a number of key clinical roles exist, and clinical support in mature wraparound communities is very strong. Rider and Penrod (2004) described key roles for clinicians in the process, adapted by VVDB with the author’s permission
Assessment and Clinical Formulation for Wrap Planning • Often, a clinician is an early referral contact for a family, already doing some service coordination at the pre-wraparound level • Provides assessment and clinical input about the process to an individual family • Helps inform the comprehensive assessment (strengths, needs and culture discovery) (Rider and Penrod, 2004)
Consultant to CPT/Wrap Staff 24 • Provide clinical advice and consultation to the Wraparound Staff • This consultation is a process function; decisions are still made in a team manner (Rider and Penrod, 2004)
Member of CPT/Wrap Team 25 • Provide clinical advice and consultation to the CPT/Wrap Team Members, including the family • Consultation includes describing why needs might be priorities, suggesting and describing options, helping to develop action steps • Building their treatment plan on the integrated wraparound (ICP) plan (Rider and Penrod, 2004)
Active Participant on CPT Team 26 • Attends Care Planning Team (CPT) meetings according to role (core or consulting) as a vital team member • As clinical issues improve role may shift from core team member to consultant (Rider and Penrod, 2004)
Service Provider Outside of Meetings 27 • Most of wraparound happens outside of team meetings (actual implementation) • May provide direct therapy outside of CPT/wraparound team meetings, with therapy driven by the family with team input. • In this role, clinician operates in close coordination with the team in one of the three roles • In this role, clinician focuses on specific goals established through team planning (Rider and Penrod, 2004)
What’s in it for Clinicians? • Youth and families are more engaged in the process • This process involve the social and physical environment of the youth • Wraparound can address areas that can not be addressed through therapy sessions • Other team members can augment important aspects of the therapeutic process
Implications for Psychiatrists • With the national crisis level shortage of Psychiatrists, wraparound can provide additional information, support, and resources for Psychiatrists to extend their reach with a family/youth
Implications for Psychiatrists • Wrap can stabilize a family/youth enough for the Psychiatrist to do their work – “It is hard to medicate a rapidly moving object”
Implications for Psychiatrists • Wraparound, when used as part of short term stabilization focused residential care or psychiatric hospitalization, can improve effectiveness of residential treatment
Why I love MBI/PBIS Wraparound • I have seen and been involved with the transformative potential of PBIS overall • PBIS provides a focus on all students and not just the “top of the triangle” youth • PBIS/Illinois innovations changed the ways schools approach students with complex needs • PBIS/Illinois innovations focused the field on what teachers need in addition to what families and students need • PBIS focused on behavior
Goal for Montana Communities and Wraparound • No family ever has two wraparound plans • Common student identification and referral mechanisms at the community level (Integrated System of Care) • Realizing that both MBI/PBIS Wraparound have aspects that are the same, similar and different, and there are reasons for the differences.
MBI/PBIS and High Fidelity Overall Wraparound Differences • Schools and Community Agencies are very different entities • Schools are much more structured and focused on education as a primary mandate. PBIS recognizes the role of behavior in the educational mandate. MBI/PBIS Wraparound is a part of the overall PBIS model • Communities and community agencies are often not integrated in focus and mandates • High Fidelity Wraparound is a process of integration, one family/youth at a time
Draft Cross-Walk of the Two Wraparounds • Draft Cross-walk will be refined • OPI and DPHHS are actively working on integration issues • Lucille and John have collaborated for almost 22 years!