Download

1 / 130
1.31k likes | 1.65k Views
Liver II. hepatitis. There are many attributable causes of hepatitis, which include: -viruses- CMV, EBV, herpesvirus , etc -autoimmune

E N D
hepatitis • There are many attributable causes of hepatitis, which include: -viruses- CMV, EBV, herpesvirus, etc -autoimmune • The term viral hepatitis is often thought to be synonymous with diseases caused by the known hepatotropic viruses, including hepatitis viruses (HAV), B (HBV), C (HCV), D (HDV), and E (HEV)
A - picornavirus B - hepadnavirus C - flavivirus D - defective virus E - calcivirus Physically Handicapped Fellow Died Cycling
Hepatitis • Acute hepatitis(<6 months ) -It is based upon the following: • incubation period • preicteric phase- malaise , fever, fatigue, nausea muscle and joint ache etc. • icteric phase- jaundice –conjugated type • convalescence
Hepatitis Microscopically: (acute hepatitis) -hepatocyte swelling ( ballooning degeneration) - presence of apoptotic hepatocytes are known as Councilman bodies -cholestasis –due to bile plug formation -cytolysis or apoptosis -lobular disarray- due to loss of architecture -regenerative changes- hepatocyte proliferation. Severe lesions may present with confluent necrosis of hepatocytes-Bridging Necrosis
Hepatitis • Chronic hepatitis(>6 months) -continuous inflammation and necrosis The presence of Fibrosis is the hallmark of chronic hepatitis. Hence Bridging fibrosis is a characteristic finding. -other etiological factors play a an important role that contribute to the chronicity of the disease -these factors include: Wilson disease, alcoholism etc. Microscopically: it may be confined to portal tracts- known as chronic persistent hepatitis it may spillover into the adjacent parenchyma and lead to “interface hepatitis”- known as piecemeal necrosis of limiting plate
Hepatitis • M/E findings con’t: HBV type may produce a ground glass appearance- due to the accumulation of HBsAg
Hepatitis con’t • Lab findings: increased ALT/AST • Diagnosis is done by serological markers
Hepatitis • Fulminant Hepatitis: • Hepatic failure that progresses within 2-3 weeks period to hepatic encephaloparhy in the absence of chronic liver disease. • Viral hepatitis accounts for 12% of Fulminant hepatic failure. • Mainly Hep.B and HAV viruses. • Massive necrosis of contigoushepatocytes with or without accompanying inflammation. • Mortality is 80% without treatment, with renal transplant mortality drops to 35 %.
Hepatitis con’t Hepatitis A • Type of virus: ssRNA related to picornavirus • Transmission: feco-oral route • Mean incubation period: 2-4 weeks • Chronicity or carrier state: No • Clinical disease: acute hepatitis • Diagnosis: anti-HAV IgMAb’s
Hepatitis con’t Hepatitis A • This is a benign and self limited disease • Clinical disease is usually mild or asymptomatic • Factors predisposing humans to HAV include: overcrowding, poor sanitation and lack of a reliable clean water • Since viremia is transient, donated blood is not screened for
Hepatitis con’t Hepatitis A • Clinical features include: mild flu like symptoms, anorexia, abdominal pain, fever, headache, hepatomegaly • Prevention: 1)hygiene 2)passive immunization with immune serum globulin for individuals exposed to the virus or those traveling to high-exposure areas and 3) pre-exposure prophylaxis using a virus inactivated vaccine.
Hepatitis con’t Hepatitis B • Hepatitis B is a worldwide healthcare problem, especially in developing areas. An estimated one third of the global population has been infected with the hepatitis B • Prevention: vaccines and blood donor screening
Hepatitis con’t Hepatitis B serological markers
Hepatitis con’t Hepatitis C • Type of virus: ssRNAFlaviridae • Route of transmission: parenteral or sexual contact • Mean incubation period: upto 2 months • Chronicity or carrier state: yes • Clinical disease: acute or chronic hepatitis/cirrhosis/HCC • Diagnosis :PCR HCV/ anti-HCV Ab with 3rd generation ELISA
Hepatitis con’t Hepatitis C • Hepatitis C is the major cause of chronic hepatitis in the United States. HCV infections account for 20% of all cases of acute hepatitis • Patients may present asymptomatically or with subclinical disease. Persistence of infection is key in HCV infections
Hepatitis con’t Hepatitis C serological markers
Hepatitis con’t Hepatitis D • Type of virus: ssRNADeltaviridae • Transmission: parenteral or sexual • Mean incubation period: same as HBV • Chronicity or carrier state: yes • Clinical disease: acute or chronic hepatitis/cirrhosis/HCC • Diagnosis: anti-HDV IgG and IgM; HDV RNA Note: co-infection with HBV/superinfection with HBV is severe
Hepatitis con’t • HDV causes a unique infection that requires the assistance of viral particles from hepatitis B virus (HBV) to replicate and infect other hepatocytes • HBV infection must be present, in order for the development of HDV virions • Co-infected individuals recover completely, whereas, individuals with superinfection progress to severe chronic hepatitis
Hepatitis con’t Hepatitis E • Type of virus: ssRNAcalcivirus • Transmission:feco-oral • Mean incubation period: 4-5 weeks • Chronicity or carrier state: no • Clinical disease: acute hepatitis • Diagnosis: anti-HEV Ab for IgM and IgG/PCR HEV RNA • Extremely fatal in pregnant women
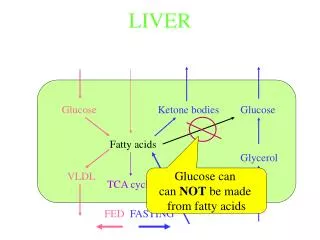
Alcoholic liver disease • Pathologic changes observed in patients with alcohol-induced liver disease can be divided into the following 3 groups: alcoholic fatty liver (hepatic steatosis), alcoholic hepatitis, and cirrhosis. • All three forms of disease may present as a spectrum of disease, or they may occur independently of one another
Alcoholic liver disease con’t • Mild and reversible changes, as seen in fatty liver, occur when an individual ingests as much as 80 g/day of alcohol • Chronic intake of alcohol of 50 -60 g/day may lead to severe forms of liver disease • Females are at an increased risk of liver disease, when compared to males • Genetics may play a role; however, no identifiable genetic markers are known
Alcoholic liver disease • Alcohol metabolism: most of the alcohol is catabolized by the several pathways, which include: • ADH – alcohol dehydrogenase • Cytochrome P-450 • MEOS- microsomal enzyme oxidation system
Alcoholic liver disease con’t Fatty liver (hepatic steatosis) • Fatty liver is the accumulation of triglycerides and other fats in the liver cells • In some patients, this may be accompanied by hepatic inflammation and liver cell death • Alcoholic fatty liver is an early and reversible consequence of excessive alcohol consumption
Alcoholic and drug related liver disease Fatty liver (hepatic steatosis) There is a defect in fatty acid oxidation and lipoprotein synthesis. This leads to peripheral conversion of fat and subsequent hyperlipidemia • Grossly: large, yellow, greasy liver • Microscopically : macrovesicular globules (lipid accumulation within the hepatocyte displaces the nucleus to the periphery)
Alcoholic liver disease Fatty liver (hepatic steatosis) con’t • Lab findings: increased bilirubin and ALP • Clinical findings: hepatomegaly • Treatment: cessation of alcohol
Alcoholic liver disease Gross: fatty liver Enlarged, yellow, greasy liver
Alcoholic liver disease M/E: Two patterns of hepatic steatosis are recognized: (1) microvesicularsteatosis: the cytoplasm is replaced by bubbles of fat that do not displace the nucleus; and (2) macrovesicularsteatosis: the cytoplasm is replaced by a large bubble of fat that displaces the nucleus to the edge of the cell.
Alcoholic liver disease Alcoholic hepatitis aka steatohepatitis • Alcoholic hepatitis is a syndrome of progressive inflammatory liver injury associated with long-term heavy intake of ethanol- up to 2 decades • The MEOS system forms the reactive oxygen species (ROS) release cytokines i.e. TNF, IL-6, IL-8, IL-18 • The combination of acetaldehyde and ROS leads to hepatic injury especially in the centrilobular region
Alcoholic liver disease Alcoholic hepatitis con’t • Microscopically • Hepatic swelling (ballooning) and necrosis • Mallory bodies- intermediate filaments and proteins appear as eosinophiliccytoplasmic inclusions • Neutrophil infiltration- these are present around degenerating hepatocytes • Perivenular fibrosis
Alcoholic liver disease Alcoholic hepatitis • Grossly: red and mottled liver • Lab findings: increased ALP/ bilirubin / AST/ ALT • Clinical findings: malaise, anorexia, weight loss, hepatomegaly, abdominal tenderness • Prognosis: complete cessation of alcohol may heal slowly; it may progress to cirrhosis
Alcoholic liver disease con’t M/E: The histologic findings shown include macrovesicularsteatosis, cytologic ballooning, Mallory bodies, and scattered lobular inflammation.
Alcoholic liver disease con’t M/E: Mallory body is shown within a ballooned hepatocyte.
Alcoholic liver disease Alcoholic cirrhosis • This is the irreversible form of alcoholic liver disease • It has the same features as any other cirrhosis- abnormal liver architecture, fibrosis, and vascular changes • Grossly : uniformly micronodular nodules < 0.3 cm in diameter. The liver initially is very large; it eventually transforms into a shrunken form
Alcoholic liver disease Alcoholic cirrhosis • Clinical findings: portal hypertension hepatic encephalopathy jaundice other findings thiamine and vitamin B12 deficiency • Lab findings: increased ALT/AST/bilirubin/ALP/ hypoproteinemia • AST/ALT ratio is increased to at least 2 to 1 • This usually requires liver transplantation
Alcoholic liver disease Gross: There is diffuse nodularity of the liver- micronodular cirrhosis- <3mm in size
Metabolic liver disease NAFLD,Hemochroatosis,Wilson’s Disease
Non-Alcoholic Liver Disease • NAFLD NAFLD/NASH • Non-alcoholic Fatty Liver Disease • Group of disorders with the common features of :Fatty liver and low (<20g/week)or absent alcohol consumption. • Includes: Simple hepatic steatosis, Steatosis with minor inflammation and NASH(non-alcoholic steato-hepatitis)
Non-Alcoholic Liver Disease • NAFLD/NASH • Pathogenesis :unclear • Two underlying events:1.Hepatic fat accumulation 2. Hepatic oxidative stress • The oxidative stress acts on the accumulated lipids leading to the generation of lipid peroxides and reactive oxygen species. • Simple steatosis is usually asymptomatic but NASH presents with hepatocyte injury and may lead to cirrhosis(10-20%)
Non-Alcoholic Liver Disease NAFLD/NASH • NASH • strongly associated with other components of the metabolic syndrome :Obesity, dyslipidemia, insulin resistance, hyperinsulinemia. • Lab: • Elevated AST/ALT • AST /ALT ratio less than 1.compared with alcoholic hepatitis where the ratio is between 2-2.5.
hemachromatosis • It is the abnormal accumulation of iron in parenchymal organs, leading to organ toxicity. • Males: females = 5:1(menstrual loss reduce progression in women) • The organs involved are the liver, heart, pancreas, pituitary, joints, and skin • It is the most common inherited liver disease in whites and the most common autosomal recessive genetic disorder.
Hemachromatosis • Hereditary hemochromatosis(primary) • Genetic mutations • HFE gene mutation responsible for most disease. This gene is located close to the HLA gene on chromosome 6 • HFE regulate the levels of hepcidin, which prevents iron absorption. Thus, reduced levels of hepcidin lead to increased levels of iron • Note: accumulation occurs by increased intestinal absorption of iron • Disease becomes evident over the coarse of several years. Liver iron stores approaches 20g/l in symptomatic patients.
Hemachromatosis • Secondary hemochromatosis: this is the acquired form of iron overload, which may be due to: • blood transfusions, β-thalessemia, sideroblastic anemia • Hemosiderin gets deposited in various organs.Deposition of hemosiderin without clinical disease is also referred to as hemosiderosis. • Grossly: micronodular cirrhosis