Download
1 / 17
170 likes | 335 Views
PUBLIC HEALTH IMPLICATIONS OF THE INCINERATION PROCESS – REVIEW OF THE EVIDENCE Roy M. Harrison The University of Birmingham. Overview Emissions and discharges from incineration Source – pathway – receptor relationships Evaluating the health evidence Conclusions.

E N D
PUBLIC HEALTH IMPLICATIONS OF THE INCINERATION PROCESS – REVIEW OF THE EVIDENCERoy M. HarrisonThe University of Birmingham
Overview • Emissions and discharges from incineration • Source – pathway – receptor relationships • Evaluating the health evidence • Conclusions
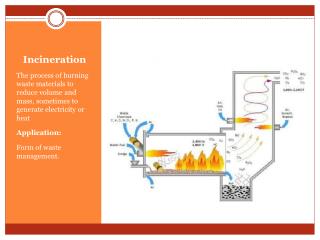
Emissions and Discharges • Incinerators emit to atmosphere • Sulphur dioxide • Oxides of nitrogen • Particulate matter (PM2.5 and PM10) • Trace metals • Toxic organic micropollutants (esp. dioxins, PCBs and polycyclic • aromatic hydrocarbons (PAH)) • Incinerators generate solid ash residues • Bottom ash • Air pollution control residues • These contain trace metals and TOMPs • Incinerators discharge cooling water • May be contaminated with trace metals and TOMPs
Abatement and Handling of Emissions • Emissions to atmosphere are much reduced due to use of abatement plant which traps much of the acidic gases, particles, trace metals and organic compounds. Dioxin emissions are also limited by adjustment of combustion conditions. • Solid waste residues (APCR) are treated as special waste and disposed to landfill. Good containment is essential. • Aquatic discharges are subject to treatment and should not offer a source – pathway – receptor risk.
Evaluating the Risk • The existence of emissions and discharges does not lead automatically to human exposure. There must be a plausible exposure pathway (a source – pathway – receptor linkage). • It is essential to distinguish between • Hazard: The potential of a substance or activity to • cause harm • Risk: The likelihood of that harm occurring
Evaluation of the Health Evidence • There are two main approaches: • To look for an excess of disease in those exposed to incinerator emissions (epidemiology); • To measure or calculate the exposures of local populations and to use exposure – response coefficients to estimate a public health impact.
Epidemiology – Establishing Causality • Epidemiology establishes statistical associations between exposure (or some other factor) and disease. This is not the same as establishing a causal link. • For epidemiological studies using a conventional 95% statistical confidence interval, one result in 20 will be positive purely by chance even if no association exists.
Potential Health Risks of Incineration • These lie in three main areas: • Cancer (various sites) • Respiratory disease • Reproductive outcomes (e.g. twins; male:female ratio; congenital abnormalities, etc.)
Epidemiological Studies of Waste Incinerators • Enviros/University of Birmingham review for DEFRA • cancer outcomes = 10 studies • respiratory disease = 6 studies • reproductive outcomes = 7 studies • Many of the studies fail to distinguish adequately between hazardous waste and municipal incinerators. • Most of the studies relate to emissions long ago when controls were far less stringent. • The studies do not present a consistent case for any adverse health outcomes being caused by incinerator emissions.
Epidemiological Studies of Waste Incinerators: The Small Area Health Statistics Unit Study • SAHSU studied cancer incidence amongst 14 million people living near 72 municipal solid waste incinerators in Great Britain over the period 1974 – 1987. • The Department of Health Committee on Carcinogenicity “was reassured that any potential risk of cancer due to residency (for periods in excess of 10 years) near to municipal waste incinerators was exceedingly low and not measurable by the most modern epidemiological techniques”.
Epidemiology relating to Incinerators • Respiratory Disease: the studies provide little evidence to conclude the incinerators cause an excess in respiratory disease. This finding is not surprising given that incremental concentrations of air pollutants due to modern incinerators are small compared to the local background levels of air pollution due to traffic and other sources. • Reproductive Outcomes: twinning, sex ratios and congenital malformations have all have studied, but the only positive results are from studies which are inconclusive, or derive from massive exposures unrepresentative of modern incinerators.
Evaluating the Health Impact: Use of Quantitative Exposure – Response Functions • The Committee on the Medical Effects of Air Pollutants (COMEAP) has used exposure – response coefficients to calculate the public health impact of the classical air pollutants in urban areas of Great Britain. • The COMEAP coefficients can, with reservations, be applied to the incremental pollution due to a point source of emissions. • World Health Organisation unit risk factors for chemical carcinogens can be applied in a similar way. • The calculations show a low level of risk associated with both the classical air pollutants and chemical carcinogens emitted from an incinerator. • e.g. Annually for an incinerator sited in an urban area • - deaths brought forward 0.008 • - respiratory hospital admissions 0.192 • - cancers (per 70 years) <0.00005 for each carcinogen
Evaluating the Health Risk: Dioxins • The prevalent expert view in the UK is that dioxins exert a carcinogenic effect through a non-genotoxic mechanism. • The implication is that there is a safe exposure level (a threshold) below which there is no cancer risk (unlike genotoxic carcinogens) • The Tolerable Daily Intake recommended by the DH Committee on Toxicity is based on the most sensitive health endpoint – reproductive and developmental effects. In their view, “it will also protect against risk of other adverse effects, including carcinogenicity”.
Do Incinerators increase the Human Body Burden of Dioxins? • Work by Fierens and co-workers (2003) indicates that • Dioxin in blood concentrations were determined in: • people residing close to an old incinerator in an industrialised • area (I-I) • people residing close to an old incinerator in a rural area (I-R) • people from an unpolluted area (No-I) • I-R group showed an elevation in dioxin levels relative to the other groups which had almost the same levels (I-I and No-I) • Extrapolation from the data indicated that a significant increase in dioxin body burden is likely to occur only when dioxin emissions exceed 5ng TEQ/Nm (c.f. the current regulatory limit of 0.1 ng TEQ/Nm ).
Conclusions • Epidemiology to date has not revealed significant public health problems with incinerators, despite focussing on an older generation of incinerators generating higher pollutant emissions. • Indirect (COMEAP-type) estimation of adverse health outcomes shows there to be only a very small health impact. • Current levels of incinerator emissions of dioxins are very unlikely to affect body burdens significantly, and no additional cancers are anticipated due to this pollutant.