Download
1 / 23
230 likes | 394 Views
2012 SURGERY. Proposal for Changes Third Year Surgery Clerkship. Surgery Clerkship. 1987 Dr. Michael Zinner arrives as new Chairman of Surgery 1992 Dr. Edward Livingston appointed Clerkship Director ,Residency Director 1993 Surgery Clerkship Partitioned:

E N D
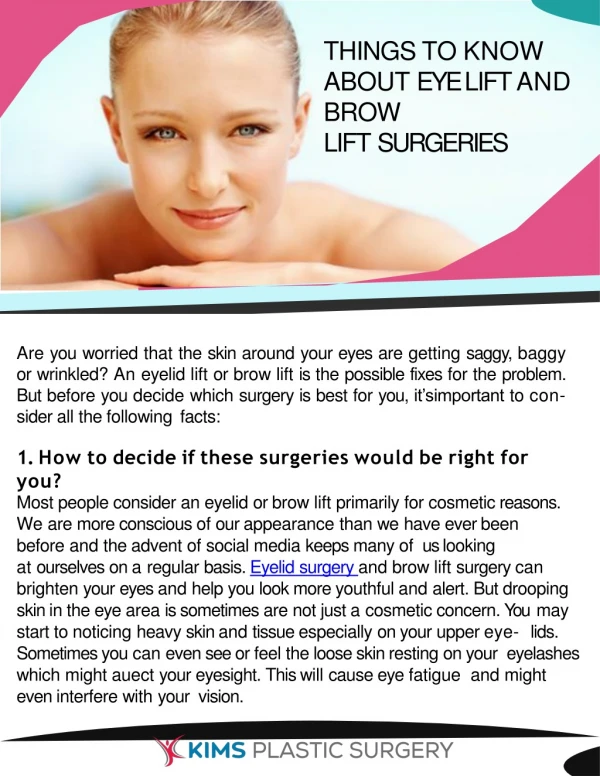
2012 SURGERY Proposal for Changes Third Year Surgery Clerkship
Surgery Clerkship • 1987 Dr. Michael Zinner arrives as new Chairman of Surgery • 1992 Dr. Edward Livingston appointed Clerkship Director ,Residency Director • 1993 Surgery Clerkship Partitioned: • Surgery I (6 weeks of 3rd Year Surgery) and • Surgery II (6 weeks of 4th Yr Surgery)
1993 Partition • 1993-4 New Surgery Clerkship implemented • Reaction from students and faculty was overwhelminglynegative • Multiple Problems: • with continuity of curriculum • students not completing required course in time for graduation • students had difficulty with separation of content
1994 Surgery 1994 • Dr. Carmak Holmes, new Chairman of Surgery, Dr. Ronald Tompkins, Vice-Chair for Education, Dr. Hugh Gelabert, Clerkship Director • Tried to make the partitioned clerkship work – to no avail • 1995 Petitioned MEC to allow Surgery Clerkship to revert to continuous 12 weeks
1994-1995 MEC • MEC - period of curricular reform • Introduction of PBL • Introduction of CPX • Introduction of standardized patients • Initiatives by California Legislature and National Political impetus to prioritize primary and ambulatory care
1995 MEC Directives • 1995 MEC Directive to strengthen physical diagnosis • Early CPX data indicated UCLA students fared poorly in several areas • Surgery Department Tasked with teaching several areas of physical exam: abdomen, vascular, ENT, orthopedic, & GU exams
1995 Surgery Proposal • 1995 Surgery Proposal: • Combined Ambulatory Surgery and In-Patient Surgery Clerkship: 6 weeks & 6 weeks to run consecutively as a 12 week block • Introduction to Surgery Week: multidisciplinary lectures and modules • Emphasis on tasked areas of physical diagnosis: Specific lectures, PE Modules
1995 Surgery Proposal • 1995 Surgery Proposal: • Revision of Surgery clerkship Curriculum to emphasize material common to all practitioners (with regard to primary care directives) • Integration of PBL into curriculum • Integration of Doctoring into curriculum • Integration of Radiology into curriculum
1995 Surgery Proposal • 1995 Surgery Proposal • Ambulatory Clerkship – 6 weeks duration • Elements: ENT, Orthopedics, Urology (per MEC tasking), Anesthesia, Ophthalmology, Plastic Surgery or Neurosurgery included in 6 rotations, each 1-week long
1995 Surgery Proposal • 1995 Surgery Proposal • General Surgery Clerkship – 6 week duration • Elements:General Surgery rotation balancing County / VA experience with Tertiary Hospital experience • 2 rotations, each 3 weeks long.
1995 Surgery Proposal • 1995 Surgery Proposal: • Additional Departmental Initiatives • Residents as Educators program • Faculty Development • Surgery Education Departmental Retreats • Surgical Education Grand Rounds, Invited Lecturers
1996 Surgery • 1995-6 Surgery Clerkship reformed and implemented • Overall reception very good • Recognition for innovation and successful implementation
2004 • Dr. Ronald Busuttil, Chairman Surgery Department • Dr. Jonathan Hiatt, Vice Chair for Surgery Education • Dr. Hugh Gelabert, Clerkship Director • Review of Clerkship and Curriculum • Review of Surgery Residency
UCLA SOM 1996-2010 PDA initiative Development of Digital education Centralization of QI data: Student Surveys Angel Educational Competencies
UCLA SOM • 2006-2009 • Implemented new curriculum for 1st and 2nd years • Implemented Colleges in 4th year • Task force to review 3rd year – Dr Hiatt
2010-12 Surgery Issues • Clerkship Problems • Evaluation and feedback cycle too long • One week rotations are too short • Difficulty integrating to clinical teams • Students seen as ‘tourists’ • Difficult to evaluate or provide constructive feedback • Some rotations are removed from central objectives of teaching core Surgery Curriculum
2012 Surgery Proposal • Surgery Clerkship Committee • Dean’s Office: Deans Wilkerson, Parker, Hiatt, Carl Stevens, Sara Kim • Anesthesia: Mitchell Lin • ENT: VishadNabili • General Surgery: Hugh Gelabert, Chris DeVirgilio, David Chen, Bryne Lee, Jessica O’Connell, Mark Sawicki, ShirinTowfigh, Darin Saltzman, Nova Foster • Neurosurgery: Isaac Yang • Ophthalmology: Gary Holland, JoAnnGiaconi • Orthopedics: Jeff Eckardt, Sharon Hame • Plastic Surgery: Charles Tseng • Transplantation: FadyKaldas • Urology: Larissa Rodriguez • Vascular: Steven Farley
2012 Surgery Proposal • Reform of Surgery Clerkship • Consolidate Subspecialties to allow more time with each rotation • Minimum duration 2 weeks, oriented towards integrated participation in services • Require participation in 2 of: Ortho, GU, ENT • Allow choice of 1 of Ophthalmology, Neurosurgery, Transplant, Cardiac, Thoracic, Plastic, Anesthesia, Ortho, GU, ENT
2012 Surgery Proposal • Revise Curriculum • Emphasis on competencies in education • Competency based reviews and exercises (Case Log, Mini-CEX, Practical Exam) • Quality Initiatives: student oriented analysis of cases and outcomes
2012 Surgery Proposal • Revise Evaluation and Feedback • Continue mid-clerkship evaluation and feedback to be given in person to students • Require ESS evaluations from specialty rotations • Continue the “Three Line” evaluation • Overall assessment • Constructive criticism • Confidential comments
Current 6 week Gen Surg 6 week Ambulatory Amb: 1 week long rotations 5 Required Subspecialties Random Assignment Proposed 6 week Gen Surg 6 week Ambulatory Amb: 2 week long rotations 2 Required subspecialties, 1 choice Student selection of assignments from 9 choices Incorporation into teams (inpatient and ambulatory) 2012 Surgery Proposal
Current ESS Evaluation at end of clerkship Separated constructive, supportive, and confidential feedback Traditional curriculum Departmental M&M sessions Proposed Mid-clerkship feedback, ESS Evaluation Separated constructive, supportive, and confidential feedback Competency based curriculum (Case Log, CEX) Content: Departmental M&M sessions, Didactics, and Online Resources 2012 Surgery Proposal
2012 Surgery Proposal • Anticipated Benefits • Improved student integration to services • Improved student participation • Improved student evaluation • Improved curriculum (competencies, QI) • Overall: Improved Educational Experience