Download
1 / 57
620 likes | 843 Views
GROUP 4 Gadin, Gonzales, Ignacio, Jumawan, Malihan, Manango, Mendoza, Morales, Oliva, Olivar. BONE MARROW, SPLEEN, LYMPH NODE, RETICULOENDOTHELIAL SYSTEM. CASE. 42-year-old male bilateral extremity edema

E N D
GROUP 4 Gadin, Gonzales, Ignacio, Jumawan, Malihan, Manango, Mendoza, Morales, Oliva, Olivar BONE MARROW, SPLEEN, LYMPH NODE, RETICULOENDOTHELIAL SYSTEM
CASE • 42-year-old male • bilateral extremity edema • (+) history ofcystic lesion in the jaw with a benign diagnosis eight years ago (see slide S-94-01) • bone pains, easy fatigability, occasional dizziness, polyuria and frequent cough and colds
The following tests were done: URINALYSIS • Protein: +++ • Glucose: + • Blood: + (intact) • Ketone: negative • Bilirubin: negative • Urobilinogen: trace • Leukocytes: +
The following tests were done: COMPLETE BLOOD COUNT • RBC: 2.2 x 106/ul • Hgb: 4.5 g/dl • Hct: 17.1% • MCV: 55 fl • MCH: 15.7 pg • MCHC: 28 g/dl • RDW: 23.6 % • WBC: 29.65 • Neutrophil: 26 • Lymphocytes:61 • Monocytes 05 • Plasma cells 05 • Eosinophils 03
Serum Protein Electrophoresis NORMAL CONTROL PATIENT SERUM
Urine Protein Electrophoresis λ β α albumin
Epidemiology • 0.8% of all cancer diagnoses (86,000 new cases)and 0.9% of cancer deaths worldwide in 2002 Bray, et al. Global Cancer Statistics, 2002 • high in North America, Australia/ New Zealand, northern Europe, and western Europe compared with Asian countries • Incidence rate including Lymphomas is479 per 1,000 WHO statistics, 2004
Source: WHO Disease incidence, prevalence and disability. 2004 retrieved fromwww.who.int/healthinfo/.../GBD_report_2004update_part3.pdf Nov 8, 2009
Epidemiology • incidence were higher among males • which is 50% higher than rates in women for all racial/ethnic groups • for FILIPINOS, the rate of incidence in men is 80% higher than women National Cancer Institute, SEER Program. 1988-1992. retrieved from http://seer.cancer.gov/publications/ethnicity/myeloma.pdf on November 8, 2009.
SEER incidence rate (1988-92) National Cancer Institute, SEER Program. 1988-1992. retrieved from http://seer.cancer.gov/publications/ethnicity/myeloma.pdf on November 8, 2009
Epidemiology • Multiple myeloma rarely occurs in the 30-54 year age group. It is commonly seen on both men and women ages 70 and above. Adam, Alexander, Cole, P., Hans-Olov, A., Mink, P., Oken, M. and Trichopoulo, D. Multiple myeloma: A review of the epidemiologic literature. 2007. Int. J. Cancer: 120, 40–61
United States MORTALITY Rates, 1988-1992 • Rates are "average annual" per 100,000 population, age-adjusted to 1970 U.S. standard; N/A = information not available • *= rate not calculated when fewer than 25 cases.
Risk Factors • There are currently no reliable or consistent predictors of risk for developing multiple myeloma, beyond race, age and sex. • Other risk factors that are being mentioned warrants further research. Adam, Alexander, Cole, P., Hans-Olov, A., Mink, P., Oken, M. and Trichopoulo, D. Multiple myeloma: A review of the epidemiologic literature. 2007. Int. J. Cancer: 120, 40–61
Risk Factors • Obesity has been associated with an elevated risk of multiple myeloma while high dietary intake of green vegetables and fish has been reported to be associated with decreased risk of the disease Adam, Alexander, Cole, P., Hans-Olov, A., Mink, P., Oken, M. and Trichopoulo, D. Multiple myeloma: A review of the epidemiologic literature. 2007. Int. J. Cancer: 120, 40–61
Risk Factors • Exposure to ionizing radiation is the only well-established risk factor for multiple myeloma, although some chemicals and occupational exposures have been reported to be associated with an increased risk Bray, F., Ferlay, J., Parkin, M., and Pisani, P. 2005. Global Cancer Statistics, 2002. CA Cancer J Clin 2005; 55:74-108
Associations between established or suspected risk factors and Multiple Myeloma Adam, Alexander, Cole, P., Hans-Olov, A., Mink, P., Oken, M. and Trichopoulo, D. Multiple myeloma: A review of the epidemiologic literature. 2007. Int. J. Cancer: 120, 40–61
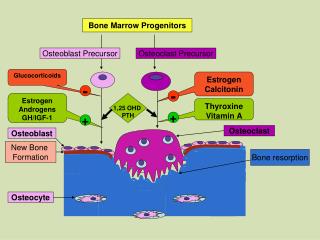
Bone pain, lytic bone lesions • Factors produced by neoplastic plasma cells mediate bone destruction, the major pathologic feature of multiple myeloma. • A variety of cytokines produced by the tumor cells, particularly MIP1α and the receptor activator of NF-κB ligand (RANKL), serve as osteoclast-activating factors Kumar, et al. 2005.
Lytic bone lesions • The bony lysis results in substantial mobilization of calcium from bone, and serious acute and chronic complications of hypercalcemia may dominate the clinical picture Braunwald et al., 2008.
Renal Symptoms • tubular damage associated with the excretion of light chains is almost always present • Normally, light chains are filtered, reabsorbed in the tubules, and catabolized.
With the increase in the amount of light chains presented to the tubule, the tubular cells become overloaded with these proteins, and tubular damage results either directly from light chain toxic effects or indirectly from the release of intracellular lysosomal enzymes
Diagnostic tests • CBC (WBC differential count) and Urinalysis • Electrophoresis (serum and urine) • Detection of the presence of tumor marker for plasma cell myeloma (Braunwald et al, 2008). • Immunoelectrophoresis • Bone marrow smear
Indications for Serum Protein Electrophoresis Suspected multiple myeloma, Waldenström's macroglobulinemia, primary amyloidosis, or related disorder Unexplained peripheral neuropathy (not attributed to longstanding diabetes mellitus, toxin exposure, chemotherapy, etc.) New-onset anemia associated with renal failure or insufficiency and bone pain Back pain in which multiple myeloma is suspected Hypercalcemia attributed to possible malignancy (e.g., associated weight loss, fatigue, bone pain, abnormal bleeding) Rouleaux formations noted on peripheral blood smear Renal insufficiency with associated serum protein elevation Unexplained pathologic fracture or lytic lesion identified on radiograph Bence Jones proteinuria
If the examination is normal but multiple myeloma, Waldenström's macroglobulinemia, primary amyloidosis, or a related disorder still is suspected, immunofixation should then be performed. This technique may be more sensitive in identifying a small monoclonal (M) protein (Kyle, 1994).
URINE PROTEIN ELECTROPHORESIS some plasma cell proliferative disorders synthesize and secrete monoclonal free light and heavy chain fragments These fragments are of relatively small molecular weight and may be readily cleared from blood To detect these abnormalities, it may be necesssary to test urine samples (Roden et al., 2008).
URINE PROTEIN ELECTROPHORESIS • is used to detect monoclonal and other proteins in the urine • monoclonal protein in serum is > 1.5 g/dL • monoclonnal free light chains are detected in serum • hypogammaglobulinemia is present in serum • serum electrophoresis shows nephrotic pattern(Brants, 2009).
IMMUNOELECTROPHORESIS also called gamma globulin electrophoresis, or immunoglobulin electrophoresis
IMMUNOELECTROPHORESIS a method of determining the blood levels of three major immunoglobulins: immunoglobulin M (IgM) immunoglobulin G (IgG) immunoglobulin A (IgA).
IMMUNOELECTROPHORESIS a powerful analytical technique with high resolving power as it combines separation of antigens by electrophoresis with immunodiffusion against an antiserum aids in the diagnosis and evaluation of the therapeutic response in many disease states affecting the immune system
Prognosis and Staging SOURCE: Fauci, 2008
Prognostic Indicators SOURCE: Multiple Myeloma Research Foundation [MMRF]. (2009). Newly diagnosed patients: what is multiple myeloma.
Other studies on serum β2-microglobulin (β2-m) level and plasma cell labeling index (PCLI) shows that β2-m >4ng/μL and PCLI >0.4% were associated with shorter survival than β2-m <1ng/μl and PCLI of 0 • (Facon et al., 2001; Gertz et al., 1989)
Deletion of chromosome13q14, 17p13 is associated with poor response to conventional induction therapy and short median overall survival (Konigsberg et al., 2000) • Recurrent translocations involving chromosome 14q32 correlate with survival as a result of intensive chemotherapy: t(4;14) is associated with short event-free and overall survival. t(11;14) associated with a longer overall survival (Moreau, et al., 2002) • Hypodiploidy (pseudodiploid, hypodiploid, near tetraploid) are adverse prognostic factors (Smadja et al., 2001)
More mature type (i.e. plasmacytic) and <20% marrow replacement are favorable, and more immature or poorly differentiated (i.e. plasmablastic) and >50% marrow replacement are unfavorable prognostic factors (Bartl et al., 1982)