Download
1 / 47
960 likes | 1.71k Views
DIAGNOSTIC METHODS IN VIROLOGY. Definition. Viruses = non cellular organisms genomes - nucleic acid, - protected by a protein shell - must replicate inside host cells. F. cannot be grown on sterile media require the presence of specific host cells Embrionated egg Cell culture

E N D
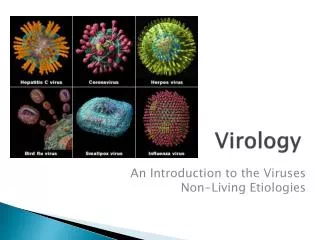
Definition • Viruses = non cellular organisms • genomes - nucleic acid, - protected by a protein shell - must replicate inside host cells
F • cannot be grown on sterile media • require the presence of specific host cells • Embrionated egg • Cell culture • Laboratory animals
DIAGNOSTIC METHODS IN VIROLOGY 3 categories: • (1) direct detection, • (2) virus isolation, • (3) serology.
1. Direct Examination of Specimen • clinical specimen - examined directly for the presence of • virus particles • virus antigen • viral nucleic acids. • Electron Microscopy morphology / immune electron microscopy • Light microscopy histological appearance - e.g. inclusion bodies • Antigen detection immunofluorescence, ELISA etc. • Molecular techniques for the direct detection of viral genomes
2. Indirect Examination = Virus isolation • Cell Culture • cytopathic effect, • haemadsorption, • confirmation by neutralization, interference, • immunofluorescence etc. • Eggs pocks - haemagglutination, inclusion bodies • Animals disease or death confirmation by neutralization
3. Serology • rising titres of antibody between acute and convalescent stages of infection, • detection of IgM in primary infection. • Classical Techniques 1. COMPLEMENT FIXATION TESTS (CFT) 2. HAEMAGGLUTINATION INHIBITION TESTS 3. IMMUNOFLUORESCENCE TECHNIQUES (IF) 4. NEUTRALIZATION TESTS 5. SINGLE RADIAL HAEMOLYSIS Newer Techniques 1. RADIOIMMUNOASSAY (RIA) 2. ENZYME LINKED IMMUNOSORBENT ASSAY (ELISA) 3. PARTICLE AGGLUTINATION 4. WESTERN BLOT (WB)
1. Direct Examination • rapid diagnostic • Result => the same/next day. • Obs: • virus isolation • serological methods May sometimes give a rapid result. !
1.1. Antigen Detection Examples – IF testing of : • nasopharyngeal aspirates for respiratory viruses • e.g.. RSV, flu A, flu B, and adenoviruses, • detection of rotavirus antigen in faeces, • detection of HSV and VZV in skin scrappings, • detection of HBsAg in serum. • Usually considered as a serological test!
1.1. Antigen Detection • main advantage: rapid (hours) • BUT technique - often tedious - result difficult to read and interpret, - sensitivity and specificity poor. • quality of the specimen - most important in order for the test to work properly.
1.2. Electron Microscopy (EM) • basis = morphology. • magnification - 50,000 X • mainly used for viral gastroenteritis • detecting viruses in feces: • rotavirus, - calicivirus • adenovirus, - Norwalk-like viruses • astrovirus, • Occasionally used for detection of viruses in skin lesions (e.g. vesicles) • herpesviruses • papillomaviruses.
1.2. Electron Microscopy (EM) • sensitivity and specificity enhanced by immune electron microscopy: • virus specific antibody used to agglutinate virus particles =>easier to recognize. • Problems with EM: • expense - purchasing and maintaining the facility. • sensitivity - often poor (106 v.particles/ml in sample required for visualization) • observer - highly skilled.
Electronmicrographs from patients suffering from gastroenteritis. From left to right: rotavirus, adenovirus, (Courtesy of Linda M. Stannard, University of Cape Town, http://www.uct.ac.za/depts/mmi/stannard/emimages.html)
Animal virus classification: DNA Viruses P o x H er p e s A d e n o P a p o v a P a rv o H e p a dn a F a mil y < -- - -- - -- - -- - -- - - - -- - -- - -- - -- - -- - -- - -- - -ds D N A -- - -- - -- - -- - -- - -- - - - -- - -- - -- - -- - -- - -- - > ssD N A P a rt i a l ds D NA G e n o m e C a ps i d C om p l e x < -- - -- - -- - -- - -- - - - -- - -- - -- - -- - -- - -- - -- - - - -- - --I co sah e d ra l - -- - -- - -- - -- - -- - -- - - - -- - -- - -- - -- - -- - -- - -- - -- - - - -- - > s y m me t ry < -- - -- - -- - -- - -- - - - Y e s-- - - - -- - -- - -- - -- - - > < -- - -- - -- - -- - -- - - - -- - -- - -- - -- - N o -- - -- - -- - -- - -- - -- - - - -- - -- - -- - - > Y e s E nv el op e Adeno- Associated Hu ma n H er p e s si m p le x P a p i l l om a H e p a t i t i s B V ac c i n i a v i r us e. g . a d e n o v i r us v ir us 2 Molluscum Contagiosum
1.3. Light Microscopy • Replicating virus => histological changes (characteristic or non-specific) in infected cells. • Viral inclusion bodies = collections of replicating virus particles (in nucleus or cytoplasm). • Examples • Babeş-Negri bodies in rabies • cytomegalic inclusion bodies in CMV infections • histology serves as an adjunct test.
RABIES VIRUS Babeş-Negri bodies in rabies
REOVIRIDAE INTRACITOPLASMATIC INCLUSIONS
INTRACITOPLASMATIC INCLUSIONS V.EBOLA HEPATOCITES
1.4. Viral Genome Detection • molecular methods • future direction of viral diagnosis • Classical molecular techniques • (dot-blot and Southern-blot) • use of specific DNA/RNA probes for hybridization • specificity depends on the conditions used for hybridization. • quantification of DNA/RNA present in the specimen • sensitivity of these techniques ~ conventional viral diagnostic methods.
1.4. Viral Genome Detection b) Newer molecular techniques: • POLYMERASE CHAIN REACTION (PCR) • LIGASE CHAIN REACTION (LCR) • NUCLEIC ACID BASED AMPLIFICATION (NASBA) • BRANCHED DNA (BDNA) PCR • extremely sensitive : 1 DNA molecule in a clinical specimen. PCR – problems: • contamination, • positive PCR result - difficult to interpret • latent viruses such as CMV !
2. Virus Isolation • Specimen - inoculated into cell culture, eggs or animals • Eggs and animals - difficult to handle • most viral diagnostic laboratories - cell culture only. 3 types of cell cultures: • Primary cells • Semi-continuous cells • Continuous cells
2.1. Types of cell cultures • Primary cells culture - e.g. Monkey Kidney. = normal cells obtained from freshly killed adult animals. (+) • best cell culture systems available • support the widest range of viruses (-) • can only be passaged once or twice. • very expensive • difficult to obtain a reliable supply.
2.1. Types of cell cultures • b. Semi-continuous cells • Human embryonic kidney • skin fibroblasts. • cells taken from embryonic tissue • passaged up to 50 times. • c. Continuous cells • HeLa, Vero, Hep2, LLC-MK2, BGM. • immortalized cells i.e. tumour cell lines • passaged indefinitely. • most easy to handle • range of viruses supported is often limited.
2.2. Identification of growing virus • a. Cytopathic Effect (CPE) - specific or non-specific • HSV and CMV produces a specific CPE, • enteroviruses do not produces a specific CPE. • b. Haemadsorption • cells acquire the ability to stick to mammalian red blood cells. • mainly used for the detection of • influenza • parainfluenzaviruses.
Left to Right: Cytopathic effect of HSV, enterovirus 71 (ballooning), and RSV in cell culture (syncytia formation) (Linda Stannard. University of Cape Town, Virology Laboratory, Yale-New Haven Hospital)
2.3 Problems with cell culture • long period for a result (up to 4 weeks) • sensitivity - often poor and depends on many factors, • condition of the specimen, • condition of the cell sheet. • very susceptible to • bacterial contamination • toxic substances in the specimen. • many viruses - not grow in cell culture at all : • Hepatitis B and C, • Diarrhoeal viruses, • parvovirus etc.
2.4 Rapid Culture Techniques • viral antigens - detected 2 to 4 days after inoculation. • Examples: shell vial cultures and the CMV DEAFF test. CMV DEAFF test • cell sheet grown on individual cover slips in a plastic bottle. • then bottle is spun at a low speed for one hour (to speed up the adsorption of the virus) • incubated for 2 to 4 days. • cover slip taken out • examined for the presence of CMV early antigens by IF (immunofluorescence)
Left: Haemadsorption of red blood cells onto the surface of a cell sheet infected by mumps virus. Also note the presence of syncytia (indistinguishable from that of RSV) (Courtesy of Linda Stannard, University of Cape Town). Right: Positive CMV DEAFF test. (Virology Laboratory, Yale-New Haven Hospital)
CELL CULTURE RECIPIENTS CELL CULTURE PH CHECKING
3. Serology = the mainstay of viral diagnosis • IgM - first antibody to appear, • IgG – follow, much higher titer • Techniques: • EIA and RIA • specifically for IgM or IgG, • most sensitive tests available • CFT, HAI => detect total antibody (comprises mainly IgG) • EIAs • better sensitivity, specificity and reproducibility than classical techniques ( CFT and HAI. )
3. Serology 3.1. Criteria for Primary Infection • a. Significant rise in titre of IgG/total antibody • acute - convalescent sera • CFT and HAI: 4 X or greater • Problem: dg. = retrospective b. Presence of IgM - EIA, RIA, and IF • rapid • Problems: • interference by rheumatoid factor, • re-infection by the virus, • unexplained persistence • Seroconversion = changing from a previously antibody negative state to a positive state. • HIV following a needle-stick injury, • antirubella following contact with a known case.
3.2. Criteria for diagnosing re-infection/re-activation • difficult to differentiate re-infection/re-activation • important under certain situations • rubella or toxoplasma infection • first trimester of pregnancy: • primary infection - high risk of fetal damage • re-infection not associated with a high risk of fetal damage • sharp large rise in antibody titres found in re-infection • IgM usually low or absent in cases of re-infection/re-activation.
Serological events in primary infection and reinfection. • Reinfection: IgM absent or only present transiently at a low level.
3.3. Limitations • Rubella and hepatitis A: • onset of clinical symptoms - development of antibodies => detection of IgM or rising titres of IgG = active disease. • Many viruses (respiratory and diarrhoeal): • clinical disease before the appearance of antibodies => serological diagnosis = retrospective • Some viruses (HIV and rabies): • clinical disease months or years after seroconversion => the mere presence of antibody is sufficient to make a definitive diagnosis.
CFT in Microtiter Plate. • Rows 1 and 2: acute and convalescent phase serum specimens, respectively. • The observed 4-fold increase is significant and indicates infection.
Microplate ELISA: • coloured wells indicate reactivity • darker the colour, higher the reactivity
3.4. Antibody in the CSF • healthy person - little or no antibodies in CSF. • viral meningitis or encephalitis, • antibodies - produced by lymphocytes • finding of antibodies in the CSF • significant when ratio between the titre of antibody in the serum and that in the CSF is less than 100 (depend on an intact blood-brain barrier !)