Download
1 / 30
300 likes | 478 Views
HT in Slovenia in the last decade - risks and benefits. Damir Franić MD PhD, Slovenia Prof. Helena Meden-Vrtovec MD PhD, Slovenia Ivan Verdenik PhD, Slovenia. VI Hrvaško-slovenski simpozij o menopavzi in andropavzi – Brijuni, 08.-11.09.2011. HT – the story of “bipolar disorder”.

E N D
HT in Slovenia in the last decade - risks and benefits Damir Franić MD PhD, Slovenia Prof. Helena Meden-Vrtovec MD PhD, Slovenia Ivan Verdenik PhD, Slovenia VI Hrvaško-slovenski simpozij o menopavzi in andropavzi – Brijuni, 08.-11.09.2011
HT – the story of “bipolar disorder” Observational studies - NHS R. Wilson. – “Feminine forever” ? 2002 1960 1963 1970 1980 1990 2011 Unopposed E, endometrial hyperplasia atypical hyperplasia, endom. Ca RCT - WHI
Post WHI era Pre WHI eraBenefits and risks of HT • Symptomrelief (QoL) • Urogenital atrophy • Osteoporosis • Cardiovascular • Neuro-cognitive • Colorectal cancer Risks Benefits • Breast cancer • Endometrial cancer • Thromboembolism • Gallbladder disease
Strength of Recommendation Decreased RR Vasomotor Symptoms Genitourinary Symptoms Cardiovascular Disease Hip and Vertebral Fracture Alzheimer’s Disease Colorectal Cancer Tooth Loss Breast Cancer Mortality Death < Age 80 A A A A BB B B B Evidence-Based Benefits of ERT Level of Evidence I II-2 II-2 II-2 II-2 II-2 II-2 II-2 II-2
Level of Evidence Strength ofRecommendation Increased RR Endometrial Cancer II-2 A VTE II-2 B Breast Cancer Diagnosis II-2 C2 Gallbladder Disease II-2 C2 Evidence-Based Hazards of ERT
Statisticaly significant cumulative incidence rates for clinical outcomes in the WHI E alone trial HR (95%CI) Favors CEE Favors placebo P value Event by Age group (y) CHD 50-590,59 (0,38-0,90) 0,05 60-69 1,00 (0,80-1,24) 70-79 1,06 (0,82-1,36) Total MI 50-590,54 (0,34-0,86) 60-69 1,05 (0,82-1,35) 0,007 70-79 1,23 (0,92-1,65) Colorectal cancer 50-590,80 (0,40-1,61) 60-69 0,90 (0,58-1,39) 0,04 70-79 1,83 (1,08-3,12) Death (all causes) 50-59 0,73 (0,53-1,00) 60-69 1,04 (0,88-1,24) 0,04 70-79 1,12 (0,94-1,33) Global index 50-590,85 (0,70-1,03) 60-69 1,00 (0,89-1,13) 0,009 70-79 1,15( 1,01-1,32) 0,4 1,0 2,0 3,0 Modified from: LaCroix et al: JAMA 2011;305(13):1305
HT “ever users” 1998 - 2007 Barbaglia G et al. Menopause 2009;16(5):1061-64
New HT users 1998-2007 Barbaglia G et al. Menopause 2009;16(5):1061-64.
HT in Slovenia – 3 points of view National Health Insurance Database (2001-2009) National Women’s Survey “Menopausis in Slovenia” (1999;2009) Slovenian Adherence Study (2003 – 2005)
National Health Insurance Database (2001-2009) No. of women age 40-65 = 349,864 Number of Prescriptions (Rp) Daily defined dose (DDD) Number of packages
Daily Defined Dose (DDD) • The basic definition of the defined daily dose (DDD) is: • The DDD is the assumed average maintenance dose per day for a drug used for its main indication in adults. • A DDD will only be assigned for drugs that already have an ATC code
“Current users” and “Ever users” • Evaluation that at least one HT prescription was prescribed – “ever users” (3 months of HT use) • Evaluation that at least two HT prescriptions were prescribed – “current users” – (6 months of HT use)
Local HT, patch, and tibolon use from 2001-2009 in Slovenia(No. of package )
Local HT, patch and tibolon use from 2001-2009 in Slovenia (DDD)
CC, SC, SCy HT use in Slovenia from 2001 – 2009 ( No. of package)
Number of prescriptions for CC, SC and SCy - % “ever users”, (“current users”) 14,3% ( 7,54%) 5,4% (2,86%)
National Women’s Survey “Menopausis in Slovenia” (1999;2009)
Slovenian Adherence Study (2003 – 2005)
Flowchart of the study. Franić D, et al, Effect of counseling on adherence to perimenopausal hormone therapy in Slovenia, Int J Gynecol Obstet (2010) in press Franić et al. Int J Gynaecol Obstet. 2010 Dec;111(3):260-3.
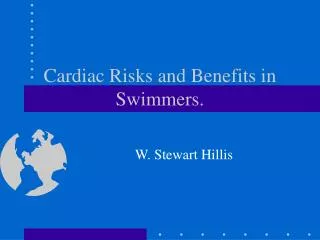
Difference in drop-outs according to time of use (14,4%) (9,7%) (54%) (44,5%) Franić et al. Int J Gynaecol Obstet. 2010 Dec;111(3):260-3.
Conclusion • The expected decrease of HT use since 2003 for systemic HT (NHID) • Stabile local HT use (NHID) • 80% satisfaction with HT (NWS) • Age of menopause in Slovenia – 52 (NWS) • Better adherence in the last decade (NWS) • Important impact of counseling on HT adherence – permanent rather than temporary (SAS) • The need to consider whether separate clinical practice guidelines should be developed for the two hormone therapy regimens.
The level of evidence by the US Preventive Services Task Force • Level I Properly randomized, controlled trial. • Level II-1 Well-designed controlled trial but without randomization. • Level II-2 Well-designed cohort or case-control analytic study. • Level II-3 Multiple time series with or without the intervention (eg, cross-sectional and uncontrolled investigational studies). • Level III Meta-analyses; reports from expert committees; descriptive studies and case reports.
WHI – Evolution of Messages From the Investigators 2002 WHI Study stopped: ‘Risks exceed benefits’. The only fundamentally new finding: ‘Substantial risks for cardiovascular disease’, in contrast to observational studies which had consistently shown reduced CHD risk in HRT users. 2003 Re-analysis: ‘[HRT] may increase the risk of CHD’. 2007 Further re-analysis: ‘Women who initiated HRT closer to menopause tended to have reduced CHD risk’. Rossouw 2002; Manson 2003; Rossouw 2007
HRT and CHD: Observational Studies and RCTs Epidemiologic Studies Age=30-55 y Time Since Menopause <6 y Randomized Trials Age <60 y Time Since Menopause <10 y 0.64 0.68 0.5 1.0 Risk Estimate Grodstein F, et al. ProgCardiovascDis 1995;38:199-210.Salpeter S, et al. J Gen Intern Med 2006;21:363-366.
Physicians practice and attitudes in post WHI era • WHI was a ground-breaking study that changed clinical practice, including counseling • Physicians varied in their opinions of HT and the scientific evidence – positive or negative • created uncertainty about the risks and benefits of HT – everybody was confused • Called for the use of decision aids • an opportunity to discuss healthy lifestyle options with patients Bush TM et al. Society of General Internal Medicine 2007;22:1311–1316