Download
1 / 32
350 likes | 850 Views
Disorders of Peripheral Arteries. Peripheral Arteriosclerosis, Arterial Embolism, & Arterial Thrombosis. Objectives. Describe pathophysiology of commonly occuring peripheral vascular disorders ID lab & diagnostic tests used to identify and assess peripheral vascular disorders

E N D
Disorders of Peripheral Arteries Peripheral Arteriosclerosis, Arterial Embolism, & Arterial Thrombosis
Objectives • Describe pathophysiology of commonly occuring peripheral vascular disorders • ID lab & diagnostic tests used to identify and assess peripheral vascular disorders • Explain nursing implications of meds prescribed for treating clients w/….. • Provide client/family teaching for clients w/common peripheral vascular disorders • Use nursing process as framework to provide individualized care to clients w/ peripheral vascular disorders
Peripheral Arteriosclerosis • Most common chronic arterial disorder • Characterized by thickening, loss of elasticity, & calcification of arterial walls • Atherosclerosis is a form of arteriosclerosis in which the thickening and hardening of the arteries are the result of deposits of fat and fibrin • In peripheral circulation, these changes result in decreased blood supply to tissues, called peripheral vascular disease (PVD) • Manifestations most common in lower extremities; 60 % or more of blood supply is occluded
Risk Factors • Over age 50 • Men > women • High-fat diet • HTN • DM • Smoking • Obesity • Stress
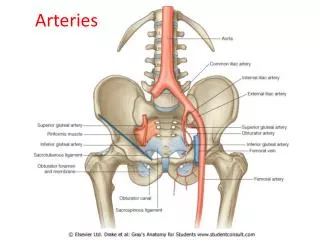
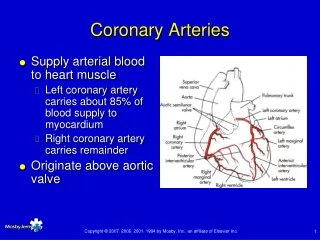
Pathophysiology: Sites of plaque deposits compromising peripheral circulation • Femoral/popliteal arteries • Common iliac arteries • Abdominal aorta • Arteriosclerosis in abdominal aorta leads to development of aneurysms as plaque development erodes vessel walls
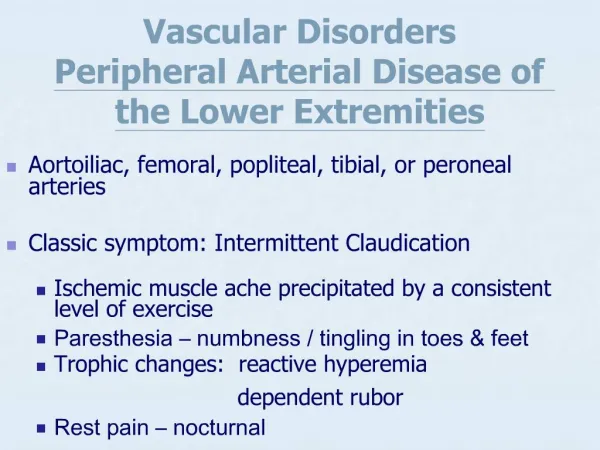
Manifestations/Complications: Pain is Primary • Intermittent claudication: cramping or aching sensation of calves of legs, thighs, buttocks; often w/limping & weakness; experienced w/activity & relieved by rest • Rest pain: often described as burning sensation in lower legs; occurs during period of inactivity; increases w/legs elevated & decreases w/legs dependent • C/O cold or numb legs • When legs are elevated, skin is pale; when legs are dependent, skin is dark red (dependent rubor) • Skin thin & shiny; areas of discoloration/hair loss, thickened toenails • Skin breakdown may lead to ulcerations & gangrene • Peripheral pulses may be decreased or not palpable
Lab & Diagnostics: Occlusive Arterial Disorders • Primarily imaging & arteriographic studies • Few lab tests are performed because interruption of arterial flow has little effect on lab values • Diagnostic tests • Segmental pressure measurements • Stress testing • Doppler ultrasonic flow study • Duplex Doppler ultrasound • Transcutaneous oximetry • Angiography or magnetic resonance angiography • Renal function studies • Oscillometry • Plethysmography
Medications • Pharmocologic mgt is less effective than w/CHD • Pentoxifylline (Trental) appears to decrease blood viscosity & increase RBC flexibility, increasing blood flow to microcirculation & tissues of extremities • Vasodilator prostaglandins may be administered parenterally to decrease pain & promote healing in clients w/ severe limb ischemia • Low doses of ASA recommended due to risk for inflammation & blood clot formation; or clopidogrel (Plavix)
Conservative Therapy • Encourage client to maintain a program of daily walking for fixed periods to promote development of collateral circulation & function. (35-45 min) • Instruct: walk to point of experiencing claudication pain, then take a 3-min rest; resume • Must stop smoking; nicotine causes vasospasm and decreases blood supply to extremities; SNS • Weight loss may decrease pain during activity
Revascularization/Surgery • Indicated w/severe intermittent claudication &/or interference w/physical activity; w/rest pain or pregangrenous lesions on foot • Nonsurgical: PTA, stent, atherectomy • Thromboendarterectomy • Arterial graft • Endovascular surgery
Nursing Process: Assessment • Complete History; Fears? • Physical Exam of lower extremities • Skin integrity • Decreased leg hair • Capillary refill of toes • Pedal pulses/Doppler ultrasound • Skin temperature • Any discolorations/infections of leg or foot • Pain assessment
Nursing Diagnosis • Ineffective peripheral tissue perfusion: Peripheral • Pain • Impaired skin integrity • Activity Intolerance
Ineffective Tissue Perfusion: Peripheral • Assess extremities for peripheral pulses, pain, color, temp, & capillary refill at least q4hrs & PRN; May need Doppler • Teach client importance of keeping extremities in a dependent position (gravity) • Keep extremities warm using lightweight blankets, socks, & slippers • Encourage change of position at least q 1 hr & avoid leg crossing • Provide thorough leg & foot care daily, using mild soap & moisturizers
Pain r/t interrupted arterial blood flow • Assess pain level using scale of 1-10 • Evaluate bilateral peripheral pulses at least q 4 hrs & more often PRN • Keep client’s extremities warm, using socks, slippers, warm blankets • Teach methods for reducing pain & relieving stress
Impaired Skin Integrity • Assess the skin of extremities at least once per shift & PRN. Document findings/changes • Provide meticulous daily skin care; keep skin clean, dry, supple • Apply bed cradle
Activity Intolerance • Assist with ADLs • Diversional activities w/bedrest • Frequent position changes/Active ROM
Teaching for Home Care • Give clients info about conservative measures that will help them manage their conditions • Teaching includes information r/t • Stress reduction • Smoking cessation • Medications:: Remember Anticoagulants • Methods of keeping extremities warm • Signs of excessive bleeding • Provide list of resources • Support groups • Public health & other community agencies • Teach leg & foot care to all family members (p. 1004)
Arterial Thrombus or Embolism • Occurs most often as complication of another disease process • Both often result in occlusion • Manifestations depend on artery involved, tissue supplied by occluded artery & degree to which collateral circulation developed • Thrombosis is usually managed w/medical tx, whereas an embolism requires immediate surgery • Focus of care: relieve obstruction & preserve extremity
Clinical Manifestations: Arterial Thrombosis • Pain in the region of the affected vessel • Numbness in the affected extremity • Pallor or mottling of skin (affected area) • Muscle spasms • No pulses distal to blockage • Possible paralysis
Clinical Manifestations: Arterial Embolism • Pain in the extremity (sudden or insidious) • Worsens w/increased extent of occlusion • Numbness in extremity • Coldness of extremity • Tingling of extremity • No pulses distal to blockage • Pallor or mottling of extremity • Muscle weakness • Paralysis • Line of demarcation, w/pallor, cyanosis, & cooler skin distal to the blockage
Lab & Diagnostics • Conducted to determine any underlying cause for thrombois or embolism & to confirm the presence of obstruction • Cardiac enzyme studies (MI?) • Blood cultures (Organism?) • Electrocardiography (ID changes of MI) • Arteriography or MRI (acute embolism) • Echocardiography (ID source of embolism)
Pharmacology • If no tissue necrosis arterial embolism or thrombosis may be treated w/thrombolytic tx using streptokinase, urokinase, or tissue plasminogen activator • Tx cannot be used if client is bleeding, has had recent surgery, uncontrolled HTN, or is pregnant • Arterial embolism may also tx w/ IV heparin as an anticoagulant
Surgery • Surgical tx of acute arterial embolus involves emergency embolectomy to prevent gangrene & to ensure adequate arterial blood flow to adjacent structures • Typical time frame is 4 to 6 hrs after embolic episode • To expedite when embolus is in extremity, may use local anesthesia • Once embolus is removed, • the area is explored for additional emboli & thrombi • Higher risk for delays >12 hrs: • Acute respiratory distress or acute • Renal failure
Nursing Care • Nursing care for client w/arterial thrombosis is essentially the same as for client w/arterial obstruction due to arteriosclerosis • Nursing Diagnoses (embolectomy or arterial reconstruction) • Anxiety • Ineffective Tissue Perfusion • Altered Protection
Anxiety Trembling, palpitations, restlessness, dry mouth, helplessness, inability to relax, irritability, forgetfulness, lack of awareness of surroundings
Anxiety • Assess level of anxiety at least once per shift & or more. Intervene to reduce current level of anxiety. • Provide opportunities for clients to verbalize anxiety, offer reassurance & support/Spend time! • Implement measures to decrease sensory stimuli. • Speak slowly and clearly • Avoid interruptions • Give concise directions • Focus on here and now • Diffuse anxiety via simple tasks
Ineffective Tissue Perfusion • Monitor lower extremities for perfusion, comparing bilaterally • Take pulses q 2-4 hrs • Take T & color of skin q 2-4 hrs • Assess capillary refill (toes) q 2-4 hrs • Be alert to c/o pain, esp if unrelieved by meds • Maintain IV fluid replacement as prescribed • Keep extremity horizontal or lower than heart • Use bed cradle to keep pressure off extremity • NO cold or heat application
Ineffective Tissue Perfusion • Avoid activities • Raising knee gatch, placing pillows under knees, avoid 90 degree hip flexion • Provide measures to promote tissue perfusion • Maintain knee of operated leg in slightly flexed position • Elevate FOB 15 degrees if lower extremity is edematous • Encourage ankle & leg exercises q 1-2 hrs while awake • Place bed cradle over lower half of bed • Keep client/environment warm
Altered Protection • Assess for & report • Excessive bloody drainage from incision • Continuous oozing from injection sites • Bleeding gums • Bleeding from nose • Hematuria • Petechiae, purpura, ecchymoses • Monitor APTT if taking heparin parentarally and PT for oral anticoagulants. Report values over target range • Monitor older adults more carefully (may require lower maintenance dose)
Teaching for Home Care • Depends on type of care needed to resolve health care problem • Preoperative teaching PRN • Pre-intra-& post op courses of therapy • Postop interventions such as meds, activity restrictions,dietary modifications, strategies for reducing atherosclerosis progression/stress reduction • D/C instructions to include S/S wound infection • Medical Mgt: conservative measures to promote peripheral circulation & maintain tissue integrity
Sample Questions • A 62-yr old client is being evaluated for a complaint of leg cramping during walking. Which of the following additional data is consistent w/intermittent claudication? • Relieved by rest • Superficial stasis ulcer over the medial ankle • Pain increases when legs are dependent • Lower leg edema
Sample Questions • Teaching for the client w/peripheral arteriosclerosis should include instructions to • Go barefoot as much as possible • Avoid excessive walking • Trim toenails weekly • Avoid tight-fitting hose or socks