Download
1 / 14
140 likes | 281 Views
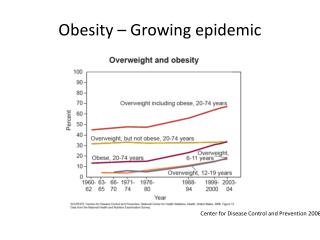
Obesity is a growing epidemic. A disease of enormous proportions >65% adults are overweight >30% adults are obese in US (Ogden et al, 2006) Associated with a number of secondary health consequences Cardiovascular disease, stroke, diabetes

E N D
Obesity is a growing epidemic • A disease of enormous proportions >65% adults are overweight >30% adults are obese in US (Ogden et al, 2006) • Associated with a number of secondary health consequences • Cardiovascular disease, stroke, diabetes (Vague et al, 1980; Gasteyger & Tremblay, 2002; Satcher, 2001)
Obesity is the result of energy imbalance Energy Expenditure Energy Intake Decreasing energy intake through diet or increasing energy expenditure through exercise is not a popular approach and has not eliminated the problem
Obesigenic Environment • Bombarded with food cues • High calorie foods are cheap and easily accessible
One successful therapy: Gastric Bypass • Roux-en-Y gastric bypass (RYGBP) • Restriction and malabsorption • Small stomach pouch near the gastro-esophageal junction and bypassing most of the stomach and duodenum • Adjustable gastric band (AGB) • Restriction • Small stomach pouch and narrow passage into the remaining stomach
RYGBP and AGB • Decrease body weight, BMI and body fat • Improvement in hyperinsulinemia, hyperleptinemia and dyslipidemia • Improvement in insulin indices (QUICKI and HOMA-IR) • Differences in ghrelin concentrations • Decrease in RYGBP • Increase in AGB
Ghrelin • Produced predominantly in the stomach (fundus) • Central and peripheral ghrelin injections to rodents and humans increases appetite and food intake • Plasma ghrelin levels rise before and fall after a meal • Plasma ghrelin levels are higher in lean or dieting individuals than obese
Why are there differences in ghrelin levels between the two procedures? • 24 Male obese patients • AGB, RYGBP and Conventional weight loss (CONV) • Matched for postoperative time, BMI, weight loss and percent body fat • 6 months after surgical procedure or CONV program blood samples were taken
What they found • Weight loss-induced increases in ghrelin levels in the AGB and CONV groups • Decreases in ghrelin in the RYGBP group • Decreases do not depend on weight loss, nutrient-related factors or insulin • Total caloric intake, macronutrient composition and insulin levels were comparable between groups • Decrease in ghrelin levels with the RYGBP depends on the surgically-induced bypass of the ghrelin producing cells of the fundus
Why do we care? • Ghrelin may enhance hedonic and incentive responses to food-related cues and thereby increase food intake • This may occur without nutritional or caloric deficiency • Non-homeostatic food intake versus homeostatic (hypothalamic) food intake • Ghrelin may contribute to the increase in obesity
Ghrelin increases brain activity in areas involved in processing food cues (Malik et al.) • 20 non-obese subjects • 3hr after ingestion of standardized meal (neither full nor hungry) • Measured cerebral response to food and non-food images (fMRI) • 12 subjects viewed pictures before and after ghrelin administration • 8 subjects viewed pictures before and after vehicle administration • Blood samples were taken before and after scan • Subjective rating for hunger were taken after each block of images
Results • Ghrelin increased activity in the amygdala, orbital frontal cortex, insula, visual areas and striatum • Not in hypothalamic areas • Ghrelin induced-increase in activation was correlated with self-reported hunger • These regions encode the salience, hedonic and incentive value of visual cues • Likely accounts for the ability of ghrelin to motivate us to eat even when we are not energy deficient
Putting these ideas together • Gastric bypass populations at Hopkins • RYGBP results in significant decreases in ghrelin • Imaging is available • Moran lab is currently doing translational work on the ability of gut peptides to alter motivation to eat and food intake
Questions • Does ghrelin contribute to the decreases in appetite and food intake in RYGBP patients? • Does exogenous ghrelin in RYGBP activate brain regions involved in reward or homeostatic (hypothalamic) areas when looking at highly palatable/hedonic food cues? • Is the ghrelin-induced brain activation after RYGBP similar to individuals pre-surgery?
Design • RYGBP patients 6 months after surgery • Is this the best time? • Blood samples to see ghrelin levels (and other factors) • fMRI imaging session following protocol of Malik et al. • Half patients will receive ghrelin, half vehicle • Test effect of ghrelin on food intake • Sucrose solution during scan? • Or separate experiment with the same patient population?