Download
1 / 93
930 likes | 1.13k Views
Management conference 18 year old man with chronic diarrhea. Raika Jamali MD Digestive Disease Research Center Tehran University of Medical Sciences. A young man with watery large volume diarrhea, 3-4 times a day from 4 months ago .

E N D
Management conference18 year old man with chronic diarrhea Raika Jamali MD Digestive Disease Research Center Tehran University of Medical Sciences
A young man with watery large volume diarrhea, 3-4 times a day from 4 months ago . Perioral paresthesia with hand & foot cramps from 3 months ago. Ulcerative lesion in the right middle & ring fingers from the same time.
Physical exam • A young man with stable vital sign & no fever. • Periorbital edema. • No icterus or anemia. No LAP. Thyroid was NL. BMI=20. • Heart & lung were NL. • There was no organomegaly or ascitis. • Exophytic lesion in distal phalanxes of the right middle & ring fingers . • Edema of lower extremities.
In the W/U for his cramps ,hypocalcemia was detected and was treated with calcium fort (4 gr/D) & rocaltrol(8000 IU/D). • The vaccination was complete. • There were no history of upper & lower respiratory tract infection or diarrhea. • Family history was negative for any recurrent infections .
LAB DATA • Giardia cyst was seen in the first S/E (which had been treated with metronidazole). • Ca=6 mg/dl 24h urinary Ca=30 mg/dl • P=3.1 mg/dl • ALP=473 • PTH=171 • Mg=2.1 mg/dl • K=3 mg/dl
NEW LAB DATA • WBC=4500 (NL Diff) • Hb=13.1 Ferritin=20 • MCV=78 Serum Iron=115 • MCH=26 TIBC=208 • MCHC=33 • Plt=249000
BUN=9 AST=39 • Cr=0.7 ALT=41 • Ca=7.5 ALP=406 • P=4 Bili direct =0.8 • Na=142 Bili direct=0.3 • K=3.8Total protein=3.6 • Mg=1.3 Albumin=1.8 • ESR=6PT=16 • FBS=108 • TG=62 ABG: metabolic Alkalosis • Cholesterol=94
S/E (3 times): Consistency=loose Ova & parasite=neg O.B=neg U/A: Normal. (without proteinuria) T4=4.9 TSH=2.5 T3=88 T3RU=36
Ig M=39 (40-200) • Ig G=200 (700-1400) • Ig A=37 (70-400) HIV Ab=neg • Anti TTG Ab=neg • Anti Endomesial Ab=neg
“25OH VIT D “ requested • Stool fat droplets with sudan 3 requested • Quantitative 72 h stool fat requested
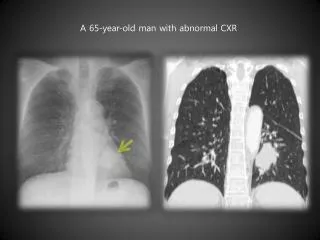
CXR: NL • WATERS VIEW: NL
Hand Radiography • Soft tissue swelling in distal part of the right middle & ring fingers . • No sign of osteomyelitis. • Diffuse osteopenia without signs of hyperparathyroidism.
Dermatology Consult • Exophytic mass in middle finger and nodular lesion in ring finger. DDx: • SCC • TB • Atypical mycobacterium • Deep mycosis • Leshmaniosis? Bx:Orf
Sonography • Liver, spleen, gall bladder, kidneys, pancreas were normal. • No ascitis. • No calcification.
Small bowel transit • Diffuse edema of mucosa. • No stricture, polyp or mass. • Ileum terminal was Nl.
Upper endoscopy Report • Esophagus: • Crico-pharyngeus , upper third, middle third and lower third were normal. • ____________________________ • Stomach: • Fundus, body, incisura and antrum were normal. • ____________________________ • Duodenum: • Bulb was normal. • ____________________________ • Additional procedures: • Multiple biopsies were takenfrom D2.
Duodenal Pathology • No Giardia. • Normal mucosal pattern without atrophy. • Adequate plasma cells in submucosa. • Dilated lymphatic ducts are seen suggesting intestinal lymphangiectasia
ABDOMINAL CT SCAN • LIVER,SPLEEN,PANCREASE AND KIDNYS WERE NORMAL. • NO ABDOMINAL LAP DETECTED.
Rectosigmoidoscopy • Anus was NL. • Rectum was NL. • Descending colon up to splenic flexure was Nl. • Bx was done.
Colon Pathology • Rectal sample was NL. • Sample of descending colon was NL.
Intestinal lymphangiectasia with protein losing enteropathy, toxic copper accumulation and hypoparathyroidism. • Aust N Z J Med. 1990 Apr;20(2):167-9
A 13-year-old girl presented with malabsorption which was ascribed to intestinal lymphangiectasia. • Three years later a generalised seizure resulted from hypocalcaemia that was shown to be due to hypoparathyroidism during investigation of which toxic copper accumulation was recognised. • The chance occurrence of three rare conditions is extremely remote making intestinal lymphangiectasia likely as the primary pathology.
It is suggested that chronic intestinal loss of the copper-carrying caeruloplasmin resulted in toxic parathyroid deposition of copper leading to hypoparathyroidism with consequent hypocalcaemic seizure.
Protein-losing gastroenteropathy • Protein-losing gastroenteropathies are characterized by an excessive loss of serum proteins into the gastrointestinal tract, resulting in : • hypoproteinemia (detected as hypoalbuminemia), • edema, • and, in some cases, pleural and pericardial effusions.
Diagnosis • The diagnosis of protein-losing gastroenteropathy should be considered in patients with hypoproteinemia in whom other causes, such as malnutrition, heavy proteinuria, and impaired protein synthesis due to liver diseases have been excluded.
PATHOGENESIS • Once plasma proteins pass into the gastrointestinal tract, they are degraded rapidly to amino acids and reabsorbed into the portal circulation. • Other serum components (eg, iron, lipids, trace elements) also may be lost in the gut.
The increase in intestinal leakage of plasma proteins can occur via one of two mechanisms: • Mucosal injury with or without erosions/ulcerations as in inflammatory bowel disease (IBD) and celiac disease. • Increased Iymphatic pressure in the gut due to granulomatous and neoplastic involvement of the Iymphatic system or after dilated lymph vessels leak protein via the surface epithelium into the gut.
The latter mechanism can occur in : • intestinal lymphangiectasia, • congenital abnormalities of the lymphatic system, • or disorders of venous stasis such as congestive heart failure or constrictive pericarditis.