Download
1 / 25
250 likes | 315 Views
A placental abruption : - pre-mature separation of normally situated placenta after 22 weeks of pregnancy. - etiology unclear. - associated factors. sever pre-eclampsia, not chronic HTN. 2. after delivery of 1 st twins ,and occurrence ROM . 3. direct trauma to the abdomen RTA.

E N D
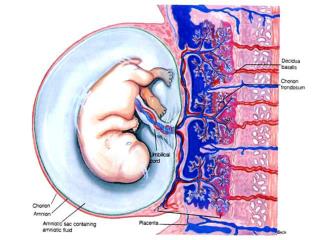
A placental abruption: • - pre-mature separation of normally situated placenta after 22 weeks of pregnancy. • - etiology unclear
- associated factors. • sever pre-eclampsia, not chronic HTN. • 2. after delivery of 1st twins ,and occurrence ROM . • 3. direct trauma to the abdomen RTA. • 4. seat belt injury • 5. violence. • 6. previous c.s • 7. High parity. • 8. cigarette smoking. • 9. ECV. • - incidence 0.4-1.8 %
* partial separation: • - bleeding from maternal venous sinus. • apparent bleeding from vaginal due to . • retained bleeding behind placenta and forced into the myometrium, and infiltrate between muscle fibers [bruised, edematous uterus] • -couvelaire uterus • -uterine apoplexy
-clp • -no vaginal bleeding. • -Signs of hypovolemic shock (concealed Hge ) • uterine enlargement. • Extreme pain.
3) Mixed Hge: • - bleeding per vagina. • - concealed Hge. In the uterine muscle. • - revealed , concealed , mixed.
* according to mother and baby condition • mild • moderate. • sever Hge. • assessing mother condition.
Hx: pre eclampsia.\recent hx of N ,V headache , blurred vision. • Physical domestic violence appear . • ECV - RTA. • Delivery of first twins • Loss of copious amount of amniotic fluid . • Slight localize pain – revealed. • - concealed (sever abd. pain.)
General examination: • Anxious , abd pain, pallor • edema of the face, fingers, pretibial area. • Alteration of v/s, except Bp in case of PIH • Respiration & pulse within normal. • Temp. :normal – air hunger • if sever infection developed fever. • Brown dark blood . • Fresh bright.
Abd examination. • More than expected gestational age concealed . • Hard uterus. • Rigid uterus, painful. • Gaurading on palpation of abdomen • Us CTG • Fetal death is common out come
assessing fetal condition : • -fetal movement • -CTG • -U\s
management: • I Vcanula , CBC , blood group , cross match ,clotting factors. • psychological care. • analgesic for pain morphine 15 mg , pethidine 100-150mg. • differentiate between pain from concealed hemorrhage, or pain from uterine contraction.
source of pain: • bleeding between muscle and membrane of placenta • labor pain • sub capsular hemorrhage ( pre -eclampsia) • management of shock (hypovolemic shock ,hemorrhagic • plasma or blood transfusion • haemacele :-doesn't alter platelet functions ,improve renal function • position left side ,sever shock elevate legs ,semi recumbent position
-midwifery role : • Resuscitate mother before surgery • Check v\s regularly • Cvp • Canula in place • I&o recorded by indwelling catheter • Urinanalysis for proteinuria • Fluid requirement should record • Fundal height checked regularly • Continuous CTG if baby living • Anti D for mother RH –ve
*management of different degree of placental abruption • 1-mild (incidental ): • Mild separation of placenta ( partial ) • Slight vaginal bleeding • Mother &fetus in stable condition
-no signs of shock • -abdomen lax • -soft uterus • -??pp • Dx: u/s • Rx:u/s • -v/s • -fetal condition monitoring by CTG • -if mother not in labor ,< 37 weeks follow up • ->37 weeks IOL
*IOL:done in case of : • 1-mild episode of bleeding • 2-no evidence of fetal compromise • Nb: anemic mother with mild abruption placenta need more concern
Moderate: • Separation of placenta 1\4 • -vaginal bleeding • -formation of retro placental blood clot • C/p: • -uterine tenderness • -increase pulse rate • -decrease blood pressure • -hypoxic baby • -IUFD
Management : • -manage shock • -analgesic • -fluid & blood transfusion • -cvp monitoring • -continuous CTG • -vaginal birth : contracted & stop bleeding after birth • -psychological support • * augmentation of labor :1-amniotomy ROM • 2-oxytocin infusion
- sever type : • -acute emergency condition • -detachment of placenta 2\3 • -life threatening condition • -most of blood concealed • -sever shock decrease blood pressure ,if normal suspect pre-eclampsia cases • -fetus almost died • -sever abdominal pain • -board like abdomen
* Complications • DIC -RF • Pituitary dysfunction • -The same as moderate treated by blood transfusion, cs delivery in case of sever bleeding • cvp • pain relief
*Care of the baby: • Asphyxia (pediatrician, equipment well prepared) • may need neonatal ICU • physical care : • full information and explanation to the family.
Partner support. • If baby go neonatal ICU "visit her" • Let mother to handle her baby before going to nursery. • N.B abruption placenta has a risk factor for recurrence in the next pregnancy.
Complications • DIC is a complication of moderate to severe placental abruption. • • Postpartum hemorrhage may occur as a result of the Couvelaire uterus and disseminated intravascular coagulation, or both. Intravenous ergometrine 0.5 mg is given at birth as a prophylactic measure. • • Renal failure may occur as a result of hypovolaemia and consequent poor perfusion of the kidneys.
Pituitary necrosis is another possible consequence of prolonged and severe hypotension (also known as Sheehan's syndrome; see medical texts for details of this rare condition). • • The maternal mortality rate due to placental abruption is 1%